Americans increasingly desire control over the timing and manner of their death. What they’re rarely told is that medicine has not yet figured out how to guarantee the peaceful ending they imagine.
The drugs used in medically assisted suicide—a cocktail of familiar medications—are given off-label in lethal doses, yet they receive sparse research.
Even when results appear predictable, the common protocols used don’t always work as expected, leaving loved ones to be witnesses to vomiting, gasping, and deaths that stretch across hours or days.
A Protocol Built on Shifting Ground
Doctors in states with medical aid in dying (MAID) laws are permitted to prescribe whatever drugs they deem fit for lethal purposes without fear of prosecution. Many rely on a protocol from the nonprofit Academy of Aid-in-Dying Medicine, although they sometimes modify it to substitute their own preferred formulations.Dr. Kerri Mason, medical director for Denver Health’s MAID program, told The Epoch Times that she personally substitutes hydromorphone for morphine to lower the volume of powder in the drug cocktail to make it more palatable.
MAID drugs are ground-up pills given in powder form to be mixed with 2 ounces of apple juice or another sweet drink to offset the bitter taste. Patients must be able to ingest the mixture themselves, although family members are permitted to mix it. They must have a terminal diagnosis with less than six months to live and be at least 18 years old.



The academy is currently working with End of Life Washington to assess a high-dose version of DDMAPh that doubles the doses of diazepam and phenobarbital for patients with opiate or benzodiazepine tolerance. Some prescribers are using the formulation for all patients.
The Data That Aren’t There
Many states are not tracking MAID data. The data that are available show that the median time to death has doubled since 2015, following the shift from single-drug protocols to combination cocktails. One patient taking the DDMAPh cocktail survived for 137 hours—nearly six days.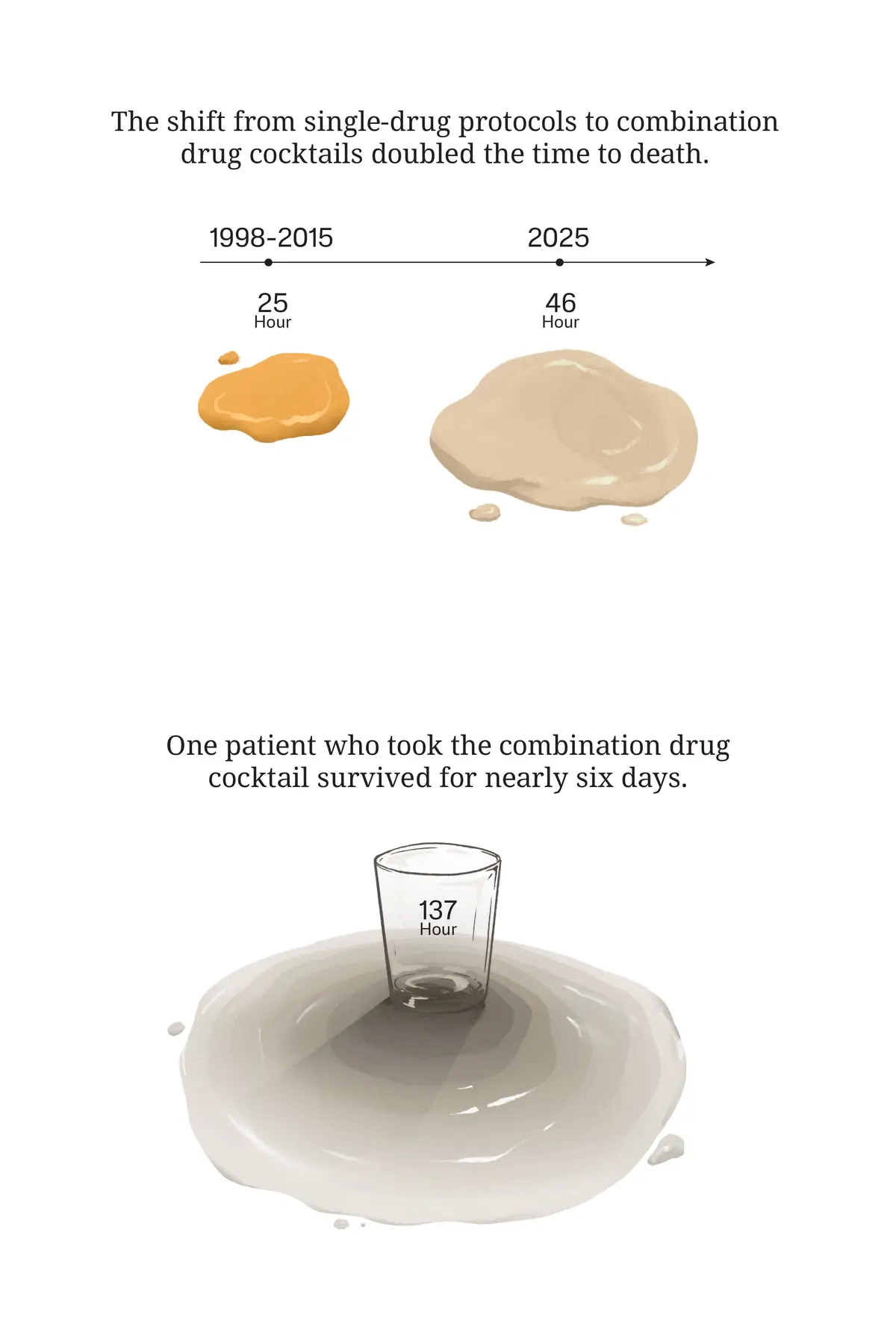
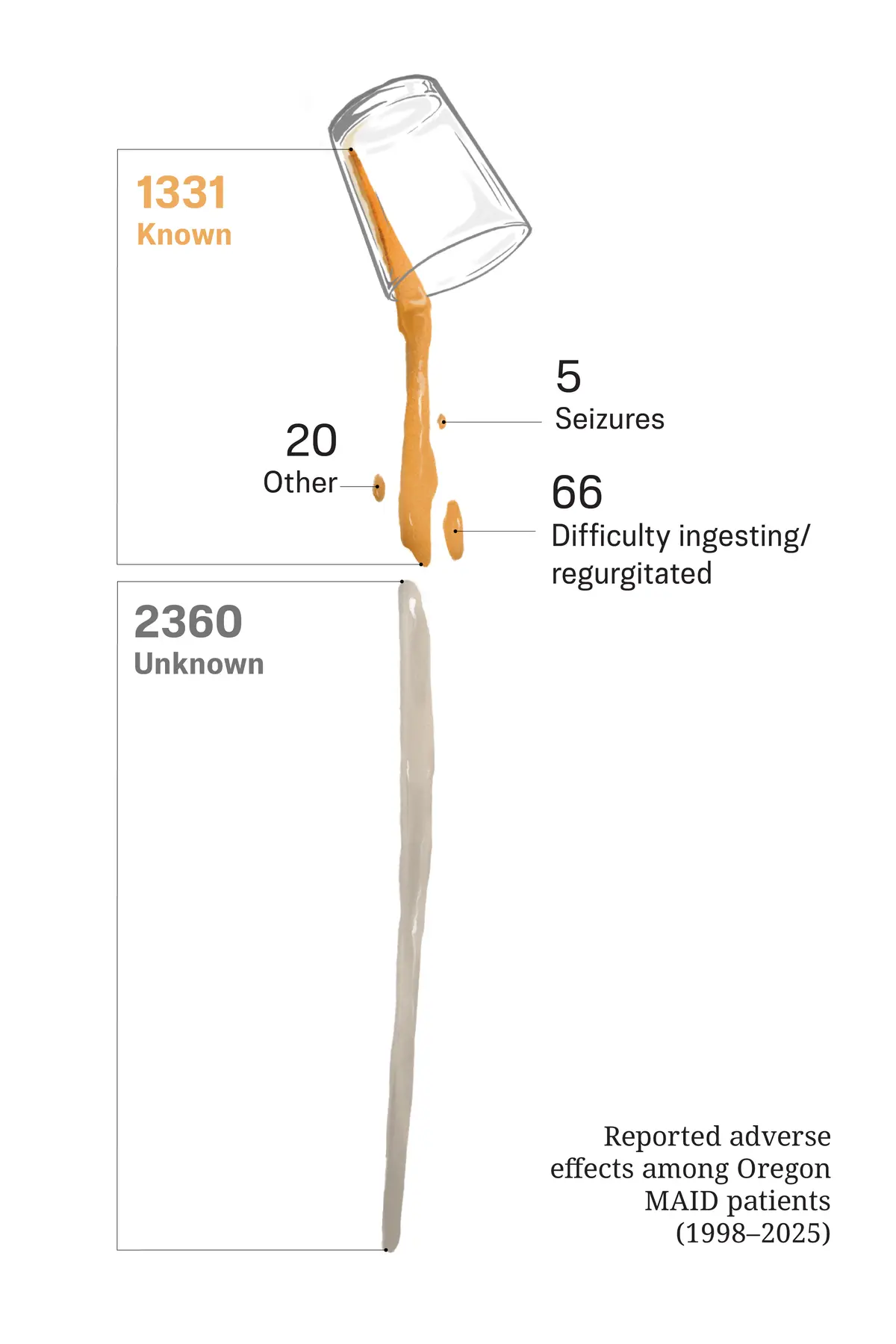
Among the nearly 1,000 cases in Oregon with known outcomes over the past two decades, five patients experienced seizures, while 66 had difficulty ingesting the medication or vomited it. From 2001 to 2025, nine people regained consciousness after ingestion. California’s 2024 report records 27 complications.
When emergency situations do arise, the response can be uncertain. California’s 2024 report notes that emergency medical services were called in three cases, a figure drawn from data covering only about half of patients who took their prescription.
Each state differs in how it collects data and what is reported, with eight states having filed up-to-date reports. Washington has suspended reports because of budget cuts. New Mexico collects information but doesn’t have public reports available, and Montana isn’t required to file reports because MAID was adopted as a result of a Montana Supreme Court action rather than legislation. Some data on the reports are unclear; for instance, the number of filed cases in New Jersey could mean prescriptions, physician attended deaths, or patients who took the drugs.
“Complications, whether a little bit of nausea or an extended onset till death, can be torturous for a patient or for loved ones,” he wrote.
One reason the data regarding MAID deaths are lacking is that healthcare providers are not required to be present for the ingestion of drugs. Some patients do not want a doctor present and prefer to die with only their loved ones present, Mason said.
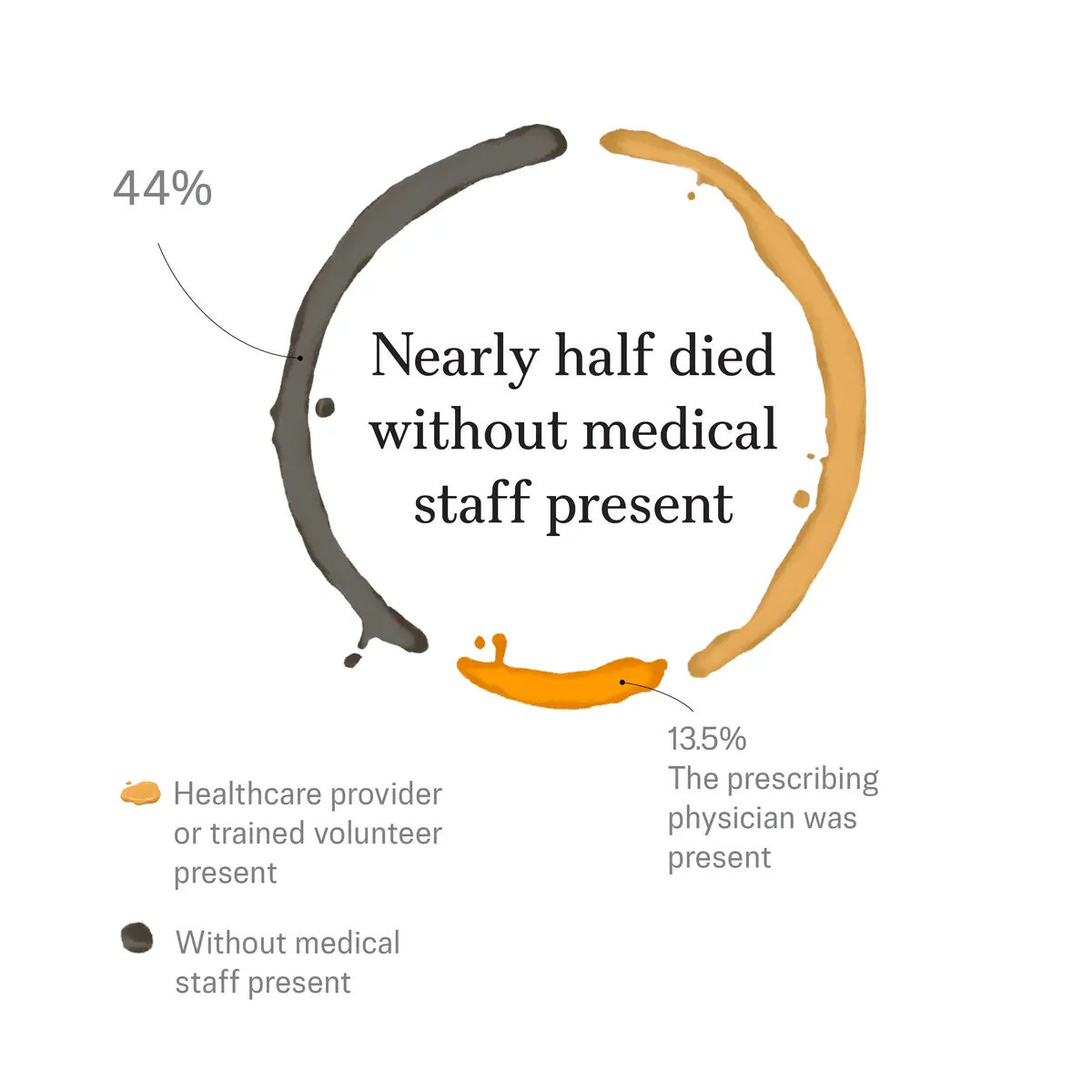
Nearly half of Oregon patients—44 percent—died without any healthcare provider or trained volunteer present. The prescribing physician was present in the room for 13.5 percent of deaths.
The British Medical Journal article found no reports of systematic monitoring of brain activity until death, blood levels of drugs, or postmortem examination of the lungs. The article went on to note that clinicians may be hesitant to reveal errors or complications.
“Despite limitations in data collection, statistics published in annual reports do reveal that ‘assisted’ deaths are not always accomplished quickly and without complication,” the authors wrote.
The lack of doctor involvement and inconsistency in data reporting reveal a deeper problem—more concern for ideologies than for science, Dr. Brick Lantz, vice president of advocacy and bioethics for Christian Medical and Dental Associations, a nonprofit organization that addresses healthcare policy issues, told The Epoch Times.
What Families See
Mason, who is sometimes present with her patients when they take their medication, is candid about the limits of prediction. She said there’s no way to predict how long it will take before somebody dies.However, those whose deaths take longer tend to be patients with abnormal metabolism—either because they were extraordinarily fit before becoming ill or because they are obese. Other cases of delayed death tend to be patients with liver disease and neurodegenerative diseases who are otherwise healthy.
Physical movements during the dying process—known as tonic movements—can alarm loved ones who aren’t prepared for them.
“That can be a little bit disconcerting, but that’s a totally normal physiologic response to hypoxia,” Mason said.
For families watching a loved one vomit or struggle to keep the medication down, the distress cuts deeper. It’s hard to know whether they’ve ingested an effective dose and if they are suffering, Lantz said.
Patients Lost in the Process
Data on patient outcomes are frequently lost in medicine because follow-up isn’t always necessary, Mason said, and MAID is no exception, especially since none of the patients are expected to live beyond a year.“Somebody either takes it or doesn’t take it and dies, and their family didn’t reach back to their provider,“ she said. ”They just kind of get lost.”
Each state has different requirements for data collected, with few reporting complications or time to death. Most reports contain only the patient’s basic demographics and three numbers: prescriptions written, deaths from ingestion, and deaths from other causes.
In Oregon, 99 patients in 2025 had an unknown outcome; they were prescribed drugs, but whether they took them or died wasn’t reported. In California, 388 patients had an unknown ingestion status in 2024.
The data gaps represent something more fundamental—a field that has moved faster than its own evidence base, Riley said. Data collection needs to be taken seriously and more research is needed, he added, while proponents should cease romanticizing complication-free deaths.
“This notion has allowed much of the general public to write them off as humane and turn a blind eye to any potential problems,” he said.