
Molly King spent six days in a diabetic coma in intensive care after she stopped taking insulin she could no longer afford.
Two nights before going to the hospital, King went to a concert and thought that she was coming down with the flu. She felt so unwell that she went to her parents’ house instead of going home. She vomited for an hour, then blacked out. In the emergency room, a nurse told her that she smelled like “Fruity Pebbles”—a classic sign of dangerously high blood sugar. Hers climbed to 1,800.
King was skipping insulin doses and stretching vials, trying to make a prescription last longer than it was ever meant to. Eventually, she stopped taking it altogether. Her doctors didn’t know. She never told them. Most patients in her situation don’t.
The Quiet Work-Arounds
King was 18 when she first learned what insulin would cost her. Newly diagnosed with Type 1 diabetes, she was still trying to grasp what it meant to need injections every day to stay alive. She had walked into the pharmacy expecting to pay for the prescription herself. Then the pharmacist quoted the price: about $400 for a month’s supply, even with insurance.She walked back to her car, opened her bank app, and called her parents in tears.
“I felt like a burden,” she said.


King’s story is extreme in its outcome but not in its shape. Across the country, patients who cannot afford a prescription do not announce the problem. They improvise—delaying, splitting, stretching, substituting, or walking away without telling the doctor who wrote the prescription.
In those work-arounds, the plan in the chart no longer matches the treatment the patient can actually follow, and harm may build for weeks before anyone notices.
Phil Cowley, a pharmacist in Utah with more than 20 years of experience, sees this play out every day.
“Patients will turn around right at the counter and leave,” he told The Epoch Times. “They don’t pick it up, and then they let everybody believe they’re taking it.”
Why Patients Stay Quiet
Speaking up about medication costs can make patients feel like failures. They may not want to admit that they cannot afford the medication. Some do not want to look irresponsible after a doctor has taken the time to explain a treatment plan. Others assume that no one can help, that the pharmacist will shrug, the doctor will move on, and the insurance company will remain as opaque as ever.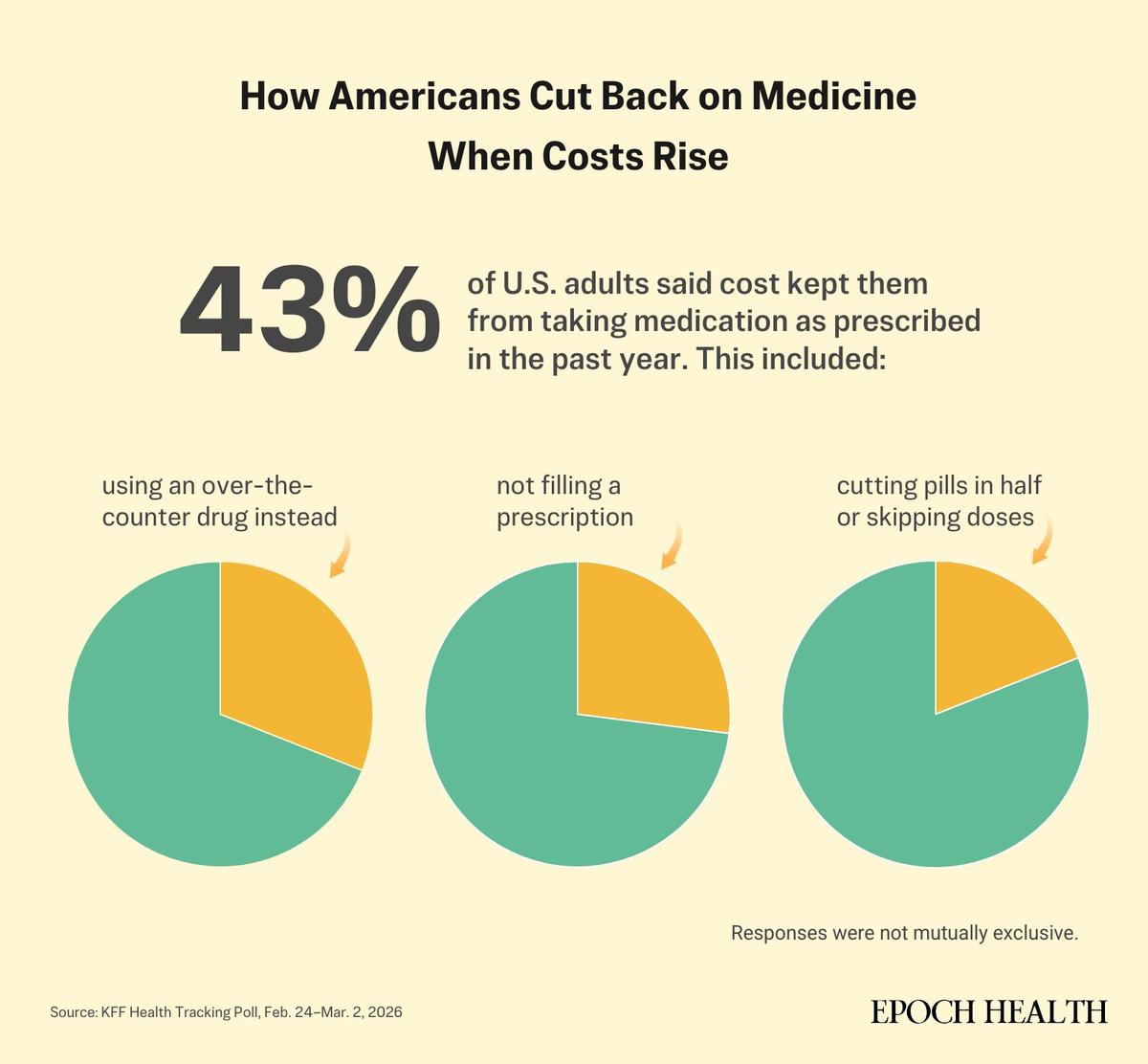
King knew that feeling firsthand.
“It feels very shameful to ask people for help with medications,” she said.
Cowley said shame is only part of it.
“I think the system has made everybody feel completely powerless,” he said.
Patients also stay quiet because they are exhausted. Those who are already sick may not have the energy to compare cash prices, call insurers, hunt for coupons, or ask whether a cheaper alternative exists. Some are managing several prescriptions at once, caring for children or aging parents, or simply trying to get through the month.
Patients for Affordable Drugs Now, which advocates for lower drug prices, told The Epoch Times that patients in its community have described cutting back on groceries, taking on credit card debt, delaying home repairs, and postponing retirement in order to keep paying for medication.
When the Plan Breaks Down
The damage from rationing is rarely visible right away, which is part of what makes it dangerous.A person with high blood pressure may skip pills and feel fine for days or weeks, even as damage builds and the risk of stroke or heart attack grows. A patient with diabetes may stretch insulin to make it last, only to watch blood sugar climb. Someone with asthma may cut back on his daily maintenance inhaler and then reach more often for the rescue inhaler because the drug meant to prevent flare-ups is no longer doing its job.
When doctors do not know that a patient has stopped, delayed, or altered a medication, they can misread the problem entirely, assuming that the drug simply isn’t working, increasing the dose, or adding another medication on top of one that was never taken in the first place.
“We see this in the emergency department, where people come in with exacerbations of heart failure, [chronic obstructive pulmonary disease], or diabetes—not because we didn’t prescribe the right medicines,” Essien said.

Cowley sees the aftermath from his side of the counter. Patients come back weeks or months later still struggling, he said, and the medical record often gives no hint that the original prescription was never filled.“No prescriptions ever work if they haven’t been taken,” he said.
Cost can shape care even before the prescription is written, Essien said. He has heard colleagues hesitate to start the best treatment because they are worried that a patient will never be able to afford it.
What to Do Before You Walk Away
The best time to start the conversation about cost is while the patient is still in the exam room.“For far too long, we’ve just kind of sent our scripts in and called it a day,” Essien said.
He described the kind of question doctors should ask more routinely: “Before we decide on our next step, I’d like to check if medication costs are ever a concern for you.”
Patients can ask for that same clarity before they leave the visit. Cowley recommends asking the prescribing doctor, “If this drug is too expensive, what are the next two acceptable alternatives?” Writing those options down gives the pharmacist clear alternatives to compare and bring back to the prescriber, rather than leaving the patient to start over at the counter.
Once the prescription reaches the pharmacy, Cowley wants patients to know the real cash price before they walk through the door by checking a coupon site or a direct-to-consumer pharmacy such as Amazon Pharmacy, GoodRx, or Cost Plus Drugs.
“You don’t go out to buy a car without already looking at the Kelley Blue Book,” he said. “You should know what the medication should cost you without insurance.”
Once you have that number, you walk into the pharmacy empowered, he said.
Cowley’s second question is even more useful: “What would you do if this was too expensive for a patient?” That question, he said, often gets better answers than a general plea for something cheaper. A pharmacist may point to a 90-day supply, a higher-dose tablet that can safely be split, or a lower-cost alternative worth discussing with the prescriber.
Cowley also urges patients to ask the pharmacist to send a message directly to the doctor: “Can you send a message to my doctor asking if we can switch to one of these other options?” That simple electronic note often gets a faster response than a phone call.






If You Still Can’t Afford It
If the price is still too high, patients still have options.Manufacturer coupons, discount cards, and patient assistance programs such as NeedyMeds or RxAssist can bring the cost down. For some conditions, disease-specific grants from organizations such as the Patient Advocate Foundation may help cover copays or even the medication itself.
Many older adults also qualify for Medicare’s Extra Help Program, a low-income subsidy that often goes unused. Direct-to-consumer pharmacies such as Cost Plus Drugs, along with coupon sites, can also lower prices, especially for generic drugs.
Patients can also check TrumpRx, the new federal discount site, to compare cash prices. It may be most helpful for people paying out of pocket before they meet their deductible, since it generally does not run through insurance.
Still, those fixes depend on patients knowing where to look and having the time and energy to keep looking. Patients for Affordable Drugs Now said that such tools help in the short term but that they do not solve the underlying problem: the price of the drug itself.
“Americans know that high drug prices are largely due to Big Pharma’s vast pricing power and its manipulation of the patent system,” Merith Basey, the organization’s executive director, told The Epoch Times in an email.
Although Medicare negotiation has produced some relief—including caps on out-of-pocket costs for Medicare patients—one in three Americans still struggle to afford prescription drugs, she said.

Why Affordable Meds Are Still Hard to Get
Patients are not shopping in a transparent market. They often have no idea what a drug will cost until they reach the pharmacy counter—and often their doctors don’t know, either. A 2021 national survey found that only 21 percent of doctors could accurately estimate a patient’s out-of-pocket drug costs even when given full information about the drug price and the patient’s insurance plan.Until transparency exists, patients will often need to advocate sooner than feels natural, while they are still well enough to ask additional questions, check the extra price, and make the hidden part of the plan visible.
A treatment only works if a patient can afford to take it.