
When you cannot speak for yourself, someone else must.
In emergency departments, operating rooms, and intensive care units, clinicians need an answer fast—often before families have grasped what’s happening. Who decides whether a new medication is started, a breathing tube is placed, or treatment continues?By the time families discuss wishes, the question is no longer whether to begin, but whether to stop.
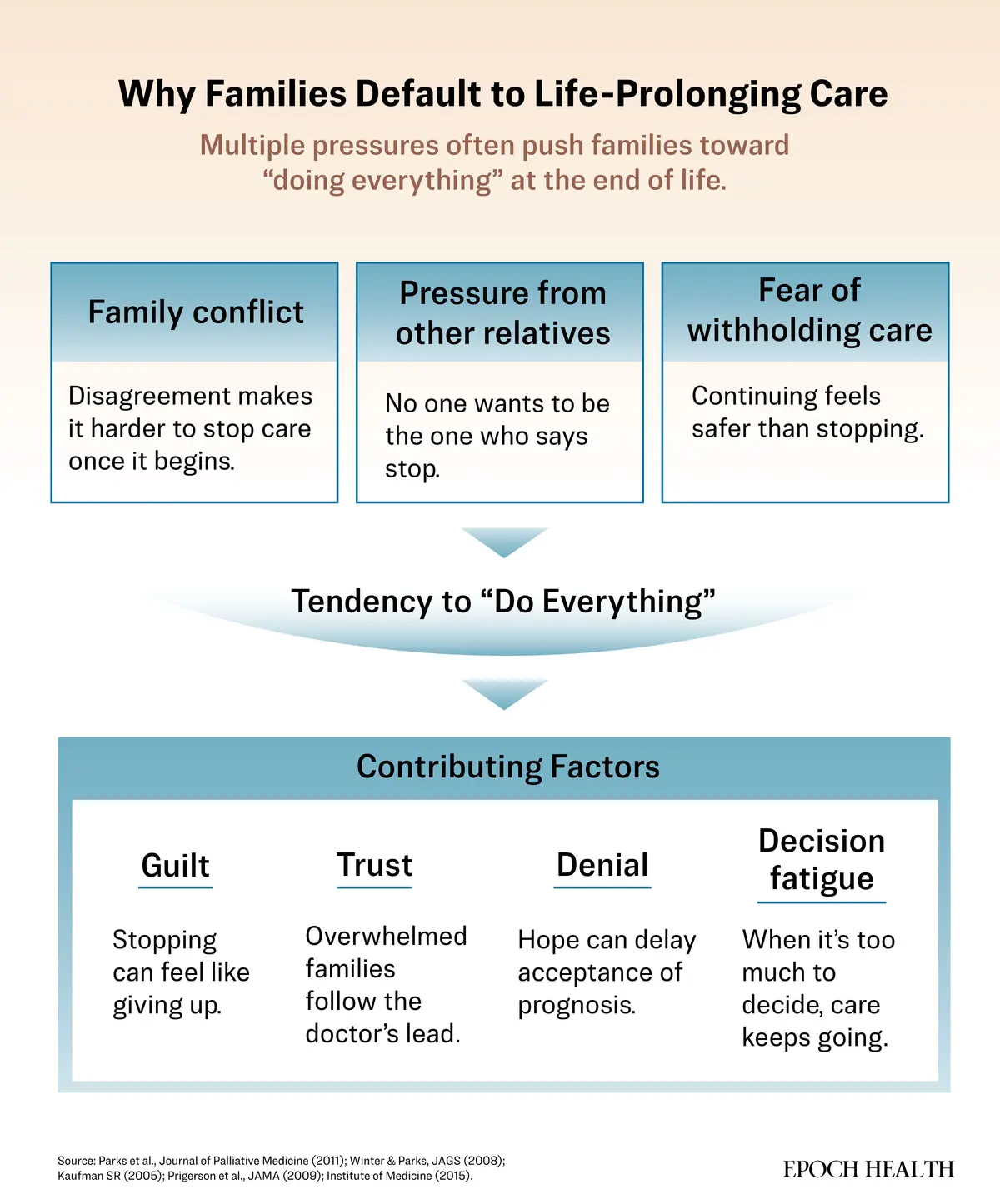
This default path carries real weight: pain, side effects, prolonged suffering, mounting costs, and the risk of treatment that overrides what the patient would have wanted or even violates their deeply held values.Why Most People Don’t Have a Proxy
A health care proxy, sometimes called a durable power of attorney for health care, names the person who can decide when you cannot. It gives one person the authority to say yes or no to what follows: which procedures are performed, which machines are used, and when care continues or stops.These decisions can shape how long you live and how much you suffer.
Only after confronting such realities does the harder question emerge—if you couldn’t speak, what would you want someone else to say for you?
There is also a quieter family cost. Choosing one person to decide may mean acknowledging that someone else will not be chosen. It can reopen old dynamics or require saying, gently, “I love you, but I need someone who can stay calm when things are uncertain.”That discomfort is precisely why the conversation matters.
What Happens Without a Proxy
Absent a proxy, most states default to surrogate laws—spouses first, then adult children, parents, or siblings. In practice, those rules often collide with real family dynamics.
Doctors may find themselves speaking with several relatives, each with a different view—one pushing aggressive treatment, another restraint, a third joining by phone with partial facts and strong opinions. Care continues amid the struggle. Disagreements can linger long after the crisis, leaving families with years of doubt and regret.
Naming a proxy prevents such situations. It is not about choosing the person who loves you most or who has the most medical knowledge, but the one who can listen, ask hard questions, and stay steady when answers are incomplete and time is short. Ultimately, it’s the person who will best honor your wishes.
Having a proxy clarifies who has authority. Naming your values asks something more personal. It forces people to consider trade-offs they hope they’ll never face—whether more time is worth the cost of dependence, whether comfort should outweigh uncertainty, whether survival at any cost still feels like living.
Why Written Values Matter
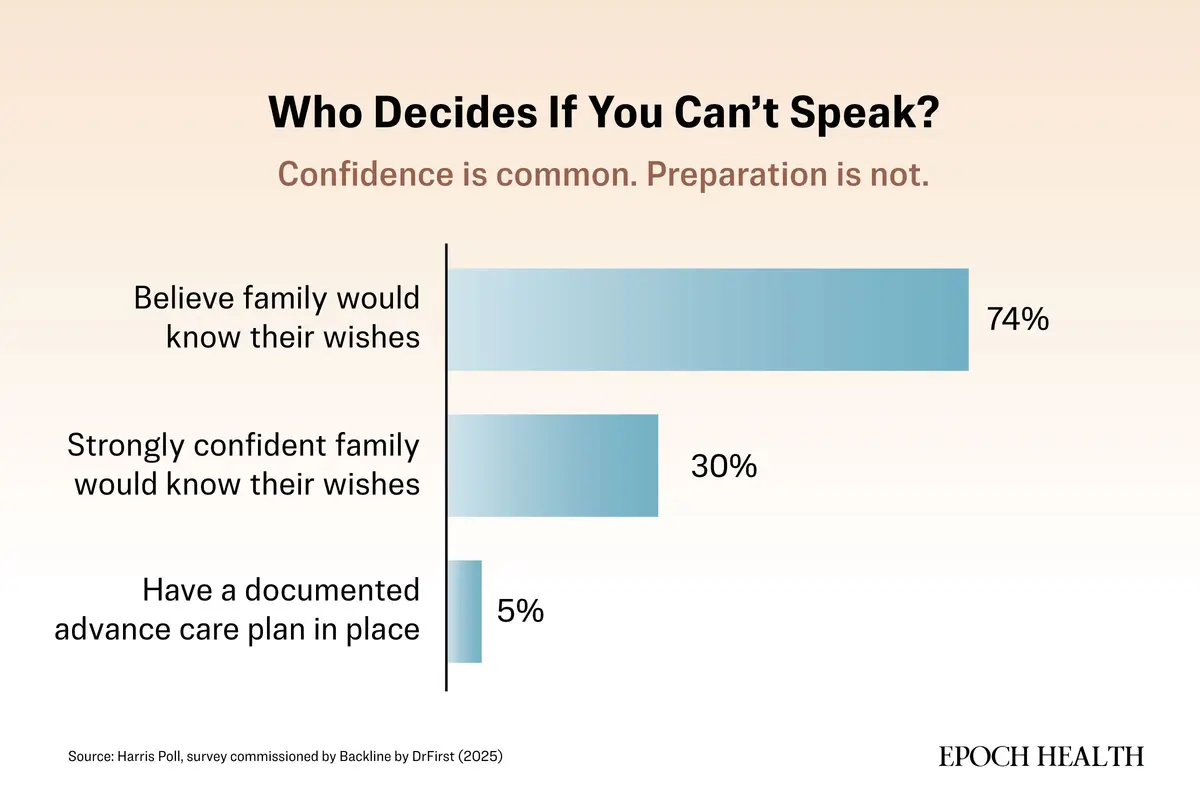
Advance directives, sometimes called living wills, capture your values—not as rigid treatment lists but as frameworks for trade-offs, reducing guesswork under stress. Most people never write a living will. A 2025 national survey found that only 5 percent of Americans have a documented, accessible advance care plan in place.Many nonetheless assume their families would know what to do. That confidence, the survey suggests, is often misplaced—only about 30 percent reported being strongly confident that their wishes would be understood and carried out.
Effective directives are concise and plain. They read less like forms and more like instructions. They clarify whether time trumps independence, comfort overrides uncertainty, or brief suffering justifies potential gains.
Why Paperwork Alone Isn’t Enough
Without discussion, advance directives invite misinterpretation. Vague terms such as “comfort-focused” or “no heroic measures” clarify little in crisis: Are antibiotics “heroic”? A feeding tube? A transfusion to get you home?Context matters. A ventilator might bridge recovery or entrench dependence; tube feeding could be temporary or permanent. Forms rarely specify “for how long” or “toward what kind of life.”
“When patients have paperwork that outlines their goals and treatment wishes but have never talked with their family or health care team about what those words mean, lots of misunderstandings occur,” Dr. Susan Nelson, a palliative care physician and president of the National POLST Collaborative, told The Epoch Times in an email.
That pattern leads to overtreatment far more often than restraint, Nelson wrote. Families default to “doing everything.” What surprises families, she added, is how quickly tentative decisions become the course of care.
Tentative steps harden into regimens. “Patients might be put on a ventilator to clear a pneumonia,” Nelson said, “when that pneumonia might be the natural end for someone with a severe, incurable illness.”
Paperwork can guide decisions. Conversation is what makes them viable.






From Preferences to Orders
In emergencies, interpretation time is scarce. Without visible orders, protocols prevail—even if families protest.Often misunderstood as care-limiting, they ensure desired treatment while avoiding unwanted ones. A comfort-focused POLST allows antibiotics, surgery, or hospitalization to relieve symptoms or to return home. A DNR or do-not-resuscitate order means no cardiopulmonary resuscitation is to be administered if the heart stops, but allows for symptom management.
Nelson recalled caring for a woman with advanced dementia. She had a comfort POLST and fractured her femur while being repositioned in bed. Nelson arranged urgent surgery so she could return home the same day and continue hospice care comfortably. She lived another six months with her family.
Navigating Systematic Hurdles
Even the most robust plans can fail if they are not accessible. Directives often exist—in offices, files, or devices—but not in emergency or operating rooms during emergencies when they are needed. Care defaults to what is immediately available.Access barriers can compound the problem. Without a Health Insurance Portability and Accountability Act (HIPAA) authorization on file, even a legally appointed proxy may be excluded from conversations or unable to review records when decisions are urgent. In fragmented health systems, clinicians may not know who the proxy is or how to reach them until it’s too late.
Planning can also become outdated. Our health changes. Relationships shift. Documents often do not. Forms completed years earlier may no longer reflect a person’s priorities, yet remain the only guidance available.
“Advance care planning isn’t something you complete once, and you’re done,” Nelson said. “It’s about talking through what matters most and revisiting those trade-offs as life or illness evolves.”
How to Have Imperative Conversations
Clinicians who study advanced care planning note that many of the most effective conversations begin informally and unfold over time, rather than during a single formal meeting.- I’ve been thinking about what matters most to me if I couldn’t speak for myself.
- What would you want for me in that situation?
- When we watched how she was cared for, what felt right to you—and what didn’t?
A Simple Place to Start
You don’t need a lawyer or a perfect plan. You need a few choices, written down, shared, and easy to find.Name a Health Care Proxy
Choose one person you trust to speak clearly under pressure. Talk with them about what matters most to you and which trade-offs you would or would not accept. Complete your state’s health care proxy form for legal validity.Write an Advance Directive
Most states offer free forms online, though a directive need not follow a specific template to be valid. Focus less on checking boxes and more on explaining your priorities in plain language. Make sure the document is properly signed in accordance with state requirements.Complete a HIPAA Authorization
A HIPAA authorization form dictates who is allowed to know what’s happening with your health care. It enables your proxy, or anyone else you designate, to receive your medical information.Make the Documents Visible
Share copies with your proxy, another contact, and your health care providers for medical upload. Keep a note on your phone or in your wallet explaining where they can be found.Revisit When Life Changes
Review your choices after major transitions, such as a new diagnosis, hospitalization, marriage, or divorce, and periodically, even when nothing feels urgent.For many people, naming and informing a proxy takes less than an hour.
With a proxy in place, if a room goes quiet, the answer is already clear.