Debbie Davis lost about 100 pounds after a bariatric surgery more than 35 years ago, but now she’s having painful symptoms that indicate the restrictive band placed on her stomach may have failed.
She cannot drink within 30 minutes of eating or she will vomit. Sometimes, she has to manually push her stomach with her hand to keep food from coming back up, and occasionally, she’ll vomit no matter what she does—even up to an hour after eating. Her throat also constantly burns from acid reflux.
“Sometimes the bloating and pain is so severe that I can hardly catch my breath,” Ms. Davis told The Epoch Times.
Surgical Failures
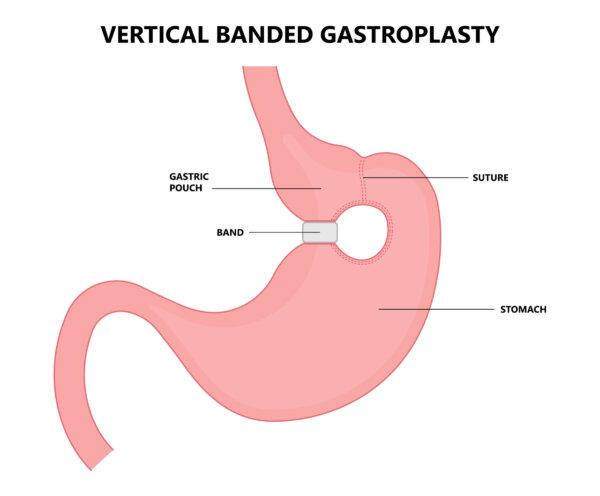
VBG surgery, which was quite popular after its 1982 introduction, has been mostly phased out because of long-term complications and the availability of more effective operations.

Ms. Davis’s situation reveals some of the problems with VBG and, to an extent, the dangers of trendy weight loss solutions that enjoy wide adoption amid early red flags. Another weight loss “solution,” known as the lap band, had a similar outcome with more than half of the bands being removed within a decade because of similar complications and weight regain.
“I see these patients every three or four years, and surgery is the only way to correct it,” Dr. Erika La Vella, a bariatric surgeon and gut health specialist with the Art of Bariatrics, told The Epoch Times. “They get a lot of weird symptoms.”
It revealed that 54 percent of those 152 cases involved a possible technical cause for surgical failure. Among those who went back for a second operation, 21 had a revised VBG, 16 had a gastric sleeve, and 115 were converted to a Roux-en-Y gastric bypass (RYGB).
A second revision procedure was documented in 16 of those patients—10 of whom converted a revised VBG to an RYGB. The clinic involved in the study stopped doing VBG revisions in 2006.
Bariatric Surgery Remains Low
Surprisingly, bariatric surgery hasn’t taken off the way it was expected to. Despite the rising rates of obesity, only about 1 percent of those who qualify for surgery choose to undergo it. About 228,000 people opt for bariatric surgery annually in the United States, according to the journal Surgery for Obesity and Related Diseases.Part of the reason is that the patient’s share of costs after insurance picks up its portion may still be prohibitive, the article reported.
As patients’ needs for additional operations grows, that might also contribute to surgical hesitancy. The possibility of revisions or secondary surgeries can make bariatric surgery even more financially daunting.
Some insurance companies won’t cover additional bariatric procedures—or they require a great deal of tests and paperwork before they’ll consider it.
“I don’t have thousands and thousands of dollars to pay for something like that when I want what I had done before fixed,” Ms. Davis said. “My whole thing is I don’t think they can fix it, but I don’t know how to get better. And there may not be any way.”
After a decade of increasing pain and several esophagogastroduodenoscopies that show that the opening to her stomach is irritated and raw, she has received no confirmation that the old surgery may be the cause.
Surgical Uncertainties
Ms. Davis is not entirely sure if her previous surgery has failed or if there’s a buildup of scar tissue around her band that’s creating additional difficulties in digestion. One surgeon wasn’t able to promise her that operating would improve her condition, only that it would help her lose weight.But she’s not obese and said what she wants most is to live out the rest of her years as healthy as she’s able.
“I felt like he was going in not knowing what he was going to find and only telling me that he was going to put another hole in my stomach so the food would go down and acid wouldn’t come back up,” Ms. Davis said. “I didn’t know if I would wake up with a feeding tube in me or exactly what might be the outcome. So I opted to forgo the surgery due to lack of information of what he was going to do so I won’t end up worse off than I was.”
The Danger of Instant Gratification
The biggest risk with bariatric treatments of all sorts is short-sighted doctors and patients, according to Dr. La Vella. In the cases of obesity, commitment to the process, long-term follow-up, and connection between the clinic and patient are vital.As a bariatric surgeon, she said she understands that most physicians are geared for instant gratification, which means getting the best possible results for patients.
“You want to deliver the operation that will help them the most but you don’t want to be so short-sighted that you don’t really project into the future—into what the long-term outcomes are like,” Dr. La Vella said. “There’s a lot of bariatric procedures put to bed a long time ago because of all their long-term nutritional complications.”
Patient selection is key, according to Dr. La Vella, who won’t work with those who can’t commit to taking supplements, getting lab work, and committing to years of appointments.
The rising rates of obesity—and more extreme cases of obesity—have put surgeons in the position to do more aggressive surgeries that were considered too dangerous a few decades ago, she said.
“We just don’t know what we don’t know, and we get too excited about quick fixes. I’m a surgeon that will just tell people, ‘No.’ It’s a tricky world to navigate,” Dr. La Vella said. “Patients who reach a level of desperation know there’s always some surgeon in the country who will do a surgery that isn’t perfectly indicated. I see that a lot.”