Bladder cancer is one of the most common cancers affecting the urinary system, and the 10th leading cause of cancer-related death in the United States. What makes it particularly notable is how treatable it can be when caught early.
Many people assume it appears without warning, but bladder cancer often announces itself through subtle signs.
What Are the Symptoms and Early Signs of Bladder Cancer?
- Pain, burning, or irritation during urination
- Sudden urgency to urinate even when the bladder is not full
- More frequent urination than usual
- Waking at night with a strong need to urinate
Symptoms of Advanced Disease
When bladder cancer becomes large or spreads beyond the bladder, it may cause more widespread symptoms, including the following:- Flank pain (pain in the side of the back, below the ribs, and above the waist)
- Abdominal pain
- Bone pain or tenderness
- Loss of appetite or unexplained weight loss
- Swelling in the feet
- Persistent fatigue
- Inability to urinate
What Causes Bladder Cancer?
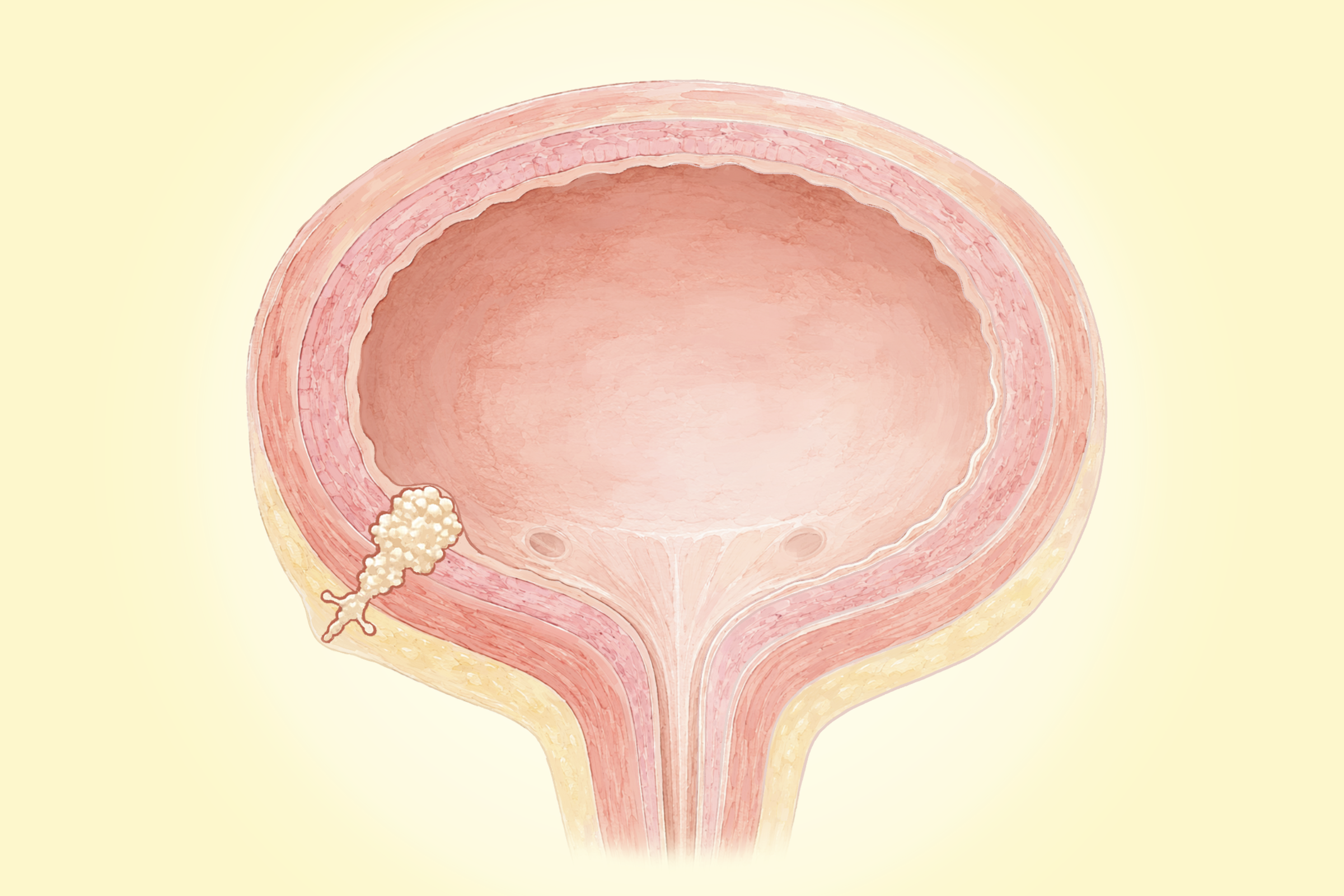
Bladder cancer develops when cells in or around the bladder begin to grow abnormally. About 90 percent of cases are urothelial carcinoma, which begins in the cells lining the inside of the bladder. In most cases, the tumor remains confined to the inner lining. Because urothelial cells also line other parts of the urinary tract—including the renal pelvis, ureters, and urethra—people with bladder cancer may also develop tumors in these areas as well. For this reason, doctors typically examine the entire urinary tract when evaluating and monitoring the disease.
Other types of bladder cancer include squamous cell carcinoma, which involves flat, skin-like cells, and adenocarcinoma, which begins in gland-forming cells.
The exact cause of bladder cancer is not fully understood, but researchers have identified several factors that increase the risk. These include genetic and other factors.
Bladder cancer develops when certain genetic mutations accumulate in genes, allowing cells to grow uncontrollably and form tumors. In most cases, these are somatic mutations, meaning they are acquired during a person’s lifetime rather than inherited. Commonly affected genes include FGFR3, PIK3CA, KDM6A, and TP53. Loss of genetic material on chromosome 9 is also frequently observed and may contribute to early disease development. These mutations can result from environmental exposures, such as carcinogens, or occur randomly.
A small number of inherited gene variants, including GSTM1 and NAT2, can reduce the body’s ability to break down harmful chemicals, increasing sensitivity to carcinogens such as tobacco smoke and industrial compounds. Certain inherited syndromes, including Lynch syndrome and Cowden syndrome, may also elevate risk.
- Smoking: Smoking is the single biggest risk factor for bladder cancer, increasing the risk by at least threefold and possibly accounting for about half of all cases. Harmful chemicals in tobacco enter the bloodstream, are filtered by the kidneys, and collect in the urine, where they come into direct contact with the bladder lining. Risk gradually decreases after quitting smoking.
- Chemical Exposure: Exposure to industrial chemicals—especially aromatic amines such as benzidine and beta-naphthylamine—has historically been used in dye manufacturing, rubber, leather, textiles, paint production, and printing. People working as painters, machinists, printers, firefighters, hairdressers, and truck drivers may face increased risk due to ongoing exposure to chemical dyes, fumes, or diesel exhaust. Because bladder cancer can take decades to develop, effects may not appear until 30 to 40 years later.
- Arsenic Exposure: Exposure to arsenic—from naturally occurring sources or industrial contamination—can increase the risk of bladder cancer when it contaminates drinking water. Arsenic is a known carcinogen that can damage DNA, impair cellular repair mechanisms, and alter gene expression.
- Medications and Supplements: The diabetes drug Pioglitazone has been linked to increased bladder cancer risk, particularly at higher doses. Supplements containing aristolochic acid—found in certain plants used in traditional herbal remedies—have also been associated with urothelial cancers, including bladder cancer, because they can cause mutational DNA damage in urothelial cells.
- Chronic Bladder Irritation and Infections: Long-term urinary tract infections, kidney or bladder stones, prolonged catheter use, and parasitic infections such as schistosomiasis have been linked to increased bladder cancer risk, particularly squamous cell carcinoma. Chronic irritation and inflammation of the bladder lining, whether from infection, stones, or injury, are thought to contribute.
- Radiation Exposure: Exposure to radiation—including radiation therapy to the abdomen or pelvis, occupational exposure, or exposure from nuclear accidents—increases the risk of bladder cancer.
- High Intake of Red and Processed Meat: Too much red and processed meat has been associated with about a 20 percent increase in bladder cancer risk. However, moderate intake of unprocessed red meat can provide essential nutrients such as protein, iron, and vitamin B12 that support overall tissue maintenance and immune function.
- Low Water Intake: Too little water intake may increase risk because regular hydration helps flush the bladder and reduces the time harmful chemicals remain in contact with the bladder lining.
- Decaffeinated Coffee: A 2025 study involving more than 120,000 participants found that men who drank decaffeinated coffee had a significantly higher risk of bladder cancer than those who did not.
- Opium Use: Although opium has medical uses for pain relief, it is also used illegally and has been linked to an increased risk of developing bladder cancer.
- Past Cancers: A personal history of urothelial cancer, such as bladder cancer, increases the risk of developing another tumor elsewhere in the urinary tract, even after the original cancer has been removed. Bladder cancer also carries a 50 percent to 80 percent risk of recurrence after treatment, either as a recurrence of the original cancer or as a new, separate cancer.
- Previous Chemotherapy: Certain chemotherapy drugs, including cyclophosphamide or ifosfamide, can irritate the bladder and increase bladder cancer risk.
- Certain Birth Defects: Rare conditions such as urachus defects and bladder exstrophy can increase the risk of bladder cancer later in life. Urachus defects involve a persistent or abnormal connection between the bladder and the belly button area, which can develop cysts or become cancerous, while bladder exstrophy occurs when the bladder does not fully close during fetal development, leaving it exposed and more prone to chronic infection and long-term cancer risk.
- Organ Transplantation: Organ transplant recipients require immunosuppressive medications, which can lead to more frequent bladder infections that are associated with a higher risk of bladder cancer.
- Age: Risk increases with age, with most cases occurring in people older than 55.
- Sex: Men are about three times more likely than women to develop bladder cancer.
- Ethnicity: Bladder cancer occurs about twice as often in white people as in African American and Hispanic populations, while Asian American populations tend to have slightly lower incidence rates, although the reasons remain unclear.
How Is Bladder Cancer Diagnosed?
Screening
Some doctors may recommend screening for people at high risk of bladder cancer using urinalysis, urine cytology, and occasionally cystoscopy.However, major medical organizations, including the American Cancer Society, generally do not recommend routine bladder cancer screening when there are no symptoms, for people at average risk, because current evidence shows that screening does not reduce mortality from the disease.
Imaging and Procedural Tests
Doctors may use imaging and procedural tests to examine the urinary tract, identify tumors, and determine whether cancer has spread.- Cystoscopy: Uses a thin, lighted tube is used to examine the bladder and urethra for tumors or other abnormalities. It can also collect biopsies or bladder washings. A fluorescent version uses a special dye and blue light to better detect cancer cells.
- Ureteroscopy: Similar to cystoscopy, but examines the upper urinary tract, including the ureters and renal pelvis.
- Biopsy/Transurethral Resection of Bladder Tumor (TURBT): Removes tumor tissue through the urethra for laboratory analysis and also serves as a primary treatment for early-stage disease.
- Intravenous Pyelogram: Uses injected dye and X-rays to image the urinary tract and detect abnormalities.
- CT Scan or CT Urography: Produces detailed images to detect tumors and evaluate whether cancer has spread.
- MRI: Provides detailed images to determine whether cancer has spread beyond the bladder.
- Ultrasound: Uses sound waves to examine nearby organs and look for signs of spread.
Blood Tests
Blood tests may help evaluate organ function and identify signs that the cancer has spread.- Kidney Function Tests: Detect possible kidney problems or blockages.
- Liver-Related Tests (Such as Alkaline Phosphatase): May indicate spread to the bones or liver.
Other Tests
Additional tests may help evaluate urinary symptoms and detect cancer-related changes in the urine.- Uroflow Test: Measures how well a person urinates by recording urine flow and the time it takes to empty the bladder.
- Urine-Based Tests: These are often used early in diagnosis. Urinalysis checks for blood, bacteria, and abnormal cells. A urine culture looks for bacteria to determine if symptoms are caused by a urinary tract infection. Urine cytology examines cells in the urine or bladder washings to detect abnormal or cancerous cells. Urine biomarker tests check for specific substances (tumor markers) in urine that may indicate bladder cancer.
Genetic Testing
Genetic testing is recommended only for select patients—particularly those diagnosed at a younger age or with a family history of related cancers, such as colon or bladder cancer. These tests identify inherited gene changes that may increase risk.What Are the Grading and Staging of Bladder Cancer?
Grading describes how abnormal cancer cells look compared to healthy cells. Low-grade cancers tend to look more like normal cells, grow more slowly, and are less likely to spread, whereas high-grade cancers appear more abnormal, grow faster, and are more likely to spread or recur. Most invasive bladder cancers are high-grade at diagnosis.
Staging refers to how advanced the cancer is and where it has spread in the body.
In stage 0 bladder cancer, the cancer is limited to the bladder lining. By stage 1, it has grown into the tissue beneath the lining but has not reached the muscle.
What Are the Treatments for Bladder Cancer?
1. Early Stage Treatments (Stages 0 & 1)
Early-stage bladder cancer is limited to the inner lining or nearby connective tissue (nonmuscle invasive), and treatment is guided by the patient’s risk group.- Surgery: Surgery is the main treatment for early-stage bladder cancer. The standard procedure is TURBT, which removes tumors through the urethra and may be the only treatment needed, although it is sometimes repeated to ensure all cancer is gone.
- Intravesical Immunotherapy or Chemotherapy: After a TURBT, early-stage bladder cancer may be treated with intravesical immunotherapy or chemotherapy, where drugs are placed directly into the bladder. Common treatments include bacterial strain Bacillus Calmette-Guérin (BCG) for immunotherapy and Mitomycin or Gemcitabine for chemotherapy. Low- or intermediate-risk cases may receive a single chemotherapy dose shortly after surgery, while intermediate- and high-risk cases often undergo a six-week course (induction therapy), especially with BCG. If successful, maintenance therapy may follow, lasting up to a year for chemotherapy or up to three years for BCG to prevent recurrence. BCG treatment may be repeated if the cancer returns or persists.
- Cystectomy: Partial or complete bladder removal may be recommended for higher-risk cases or when other treatments fail.
2. Muscle-Invasive Bladder Cancer Treatments (Stages 2 and 3)
The sequence of treatments depends on whether a bladder-preserving approach is used.- Surgery: Radical cystectomy, or the removal of the entire bladder, is the most common procedure, followed by creating a new way for urine to leave the body called urinary diversion. Lymph nodes in the pelvis are often removed (pelvic lymph node dissection) at the same time. In some cases, tumors are removed through the urethra (TURBT), especially if a bladder-preserving approach is used. Partial cystectomy, which removes only part of the bladder, is used less often as a treatment.
- Bladder Reconstructions and Stomas: After bladder removal, urine is rerouted using different reconstruction options. A urostomy (ileal conduit) creates a stoma on the abdomen where urine drains into an external bag. A neobladder uses a section of the small intestine to form an internal reservoir connected to the urethra, allowing urination through the body. A continent urinary diversion also uses a bowel-made internal pouch, but urine is drained through a stoma using a catheter rather than continuously collecting in an external bag.
- Chemotherapy: Chemotherapy is usually used before bladder removal surgery, but sometimes after or on its own if surgery isn’t possible. Treatment is usually given through a vein and typically includes cisplatin-based drug combinations.
- Radiation Therapy: Radiation may be used with chemotherapy after tumor removal, or alone if surgery isn’t possible. Radiation uses high-energy X-rays to kill cancer cells in the bladder that may not be visible during surgery, while minimizing damage to healthy tissue.
- Bladder-Preserving Approach: In some cases, TURBT followed by combined chemotherapy and radiation (chemoradiation) can spare the bladder. This is typically followed by pelvic lymph node treatment to address any hidden spread.
- Targeted Therapy: Targeted therapies attack specific molecules in cancer cells to stop their growth while minimizing damage to normal cells. Erdafitinib can be used if the cancer has FGFR2 or FGFR3 gene mutations that don’t respond to chemotherapy.
- Immunotherapy: Immunotherapy helps the immune system fight bladder cancer and may be used when cancer keeps growing after chemotherapy, comes back within a year, can’t be treated with surgery or chemotherapy, or has a high risk of recurrence. It’s often given on its own, sometimes with chemotherapy, or as maintenance therapy after chemotherapy.
3. Metastatic Bladder Cancer Treatments (Stage 4)
At this stage, treatment focuses on relieving symptoms, improving quality of life, and slowing the disease’s progression rather than curing it.- Drug combinations such as pembrolizumab with enfortumab vedotin
- Chemotherapy alone or followed by maintenance immunotherapy
- Immunotherapy alone
- Radiation combined with chemotherapy to improve effectiveness
- Surgery, including radical cystectomy or urinary diversion, to relieve symptoms or prevent complications such as urinary blockage
- Palliative care to manage symptoms and support quality of life
4. Recurrent Bladder Cancer Treatments
Treatment depends on what therapies were used before the cancer returned. Options may include systemic chemotherapy, immunotherapy drugs, or targeted therapies. In some cases, surgery may be used for localized or nonmuscle-invasive recurrence, sometimes followed by chemotherapy and immunotherapy. Radiation therapy may also be used as palliative treatment to help relieve symptoms.5. Acupuncture and Acupressure
Acupuncture and acupressure are emerging as safe complementary therapies for people undergoing urologic cancer surgery. Research suggests they can reduce perioperative pain and opioid use, help prevent or treat postoperative nausea and vomiting, and improve recovery of bowel function and oral intake, which may also shorten hospital stays.6. Cognitive Therapy
Cognitive therapy uses techniques such as deep breathing and guided imagery to help train the brain to better control the bladder without relying on medication or surgery. It can be effective in managing urge incontinence and improving overall bladder health, particularly for women.7. Emerging and Experimental Treatments
Researchers are continuing to explore newer therapies designed to target bladder cancer more precisely and improve outcomes when standard treatments are not effective.- Gene Therapy: This experimental approach alters a patient’s DNA to help fight cancer by adding healthy genes, correcting or removing faulty ones, or blocking cancer growth. In bladder cancer, it is being used in select cases where the disease has not spread into the muscle layer but does not respond to standard intravesical therapy.
- Antibody-Drug Conjugates (ADCs): These targeted therapies combine a cancer-seeking antibody with a potent chemotherapy drug, delivering it directly to tumor cells while minimizing harm to healthy cells, which helps reduce side effects. ADCs are currently approved mainly for metastatic disease, where they are given intravenously on a regular schedule and continued as long as they are effective.
What Are the Natural and Lifestyle Approaches to Bladder Cancer?
1. Diet
While there isn’t a specific diet for bladder cancer, focusing on a balanced diet can support overall health during treatment and recovery.Certain foods or supplements may also help ease treatment-related symptoms. For example, magnesium oxide, mineral water, and psyllium can help with constipation, while lean proteins can help maintain muscle strength during chemotherapy. Staying well hydrated—by drinking water or alternatives such as herbal teas or infused water is also important, although fluid needs should be discussed with a doctor.
2. Meditation and Mindfulness
A 2025 study found that combining epirubicin chemotherapy with mindfulness-based interventions may improve cancer care by reducing treatment-related side effects and psychological distress in people with urinary system tumors.3. Exercise
Exercise is positively associated with improved quality of life in bladder cancer survivors. A 2021 systematic review of 23 studies found that adopting a healthy lifestyle—including regular physical activity—may reduce the risk of developing bladder cancer and support better survivorship outcomes and overall quality of life.4. Music
A 2024 study of 160 men with bladder cancer undergoing follow-up flexible cystoscopy found that participants who listened to music with noise-canceling headphones experienced significantly lower post-procedure anxiety and higher satisfaction and willingness to repeat the procedure than those who didn’t listen to music.How Can I Prevent Bladder Cancer?
Dietary Recommendations
The following dietary recommendations may be helpful in preventing bladder cancer:- Eat more vegetables, especially nonstarchy vegetables such as leafy greens, broccoli, and peppers
- Include whole grains and dietary fiber in the diet
- Eat fish and cruciferous vegetables, which may help lower the risk
- Eat foods rich in vitamins E, C, and D
- Limit processed meats and eat a moderate amount of red meat
- Stay well hydrated
Other Tips
Additional lifestyle and environmental measures may also help lower bladder cancer risk:- Quit smoking or avoid starting
- Maintain a healthy weight
- Wear protective clothing and masks when working with harmful chemicals
- Avoid medicines and herbal remedies containing aristolochic acid.
- Avoid opium use
- Treat urinary tract infections promptly and seek medical care for kidney or bladder stones
- Limit unnecessary radiation exposure
Reducing Recurrence Risk
Some evidence suggests that taking high doses of certain vitamins and minerals—including vitamins A, B6, C, and E, along with selenium and zinc—may help reduce the risk of recurrence.What Are the Possible Complications of Bladder Cancer?
- Anemia
- Swelling of the ureters due to urine buildup
- Narrowing of the urethra
- Loss of bladder control
- Difficulty with erections in men
- Sexual dysfunction in women