What Causes PMOS?
Girls who show signs of early puberty, such as underarm or pubic hair before age 8, may be at an increased risk of developing PMOS later in life. These signs may indicate premature adrenarche, which can reflect underlying hormonal and metabolic changes linked to a higher risk of PMOS.
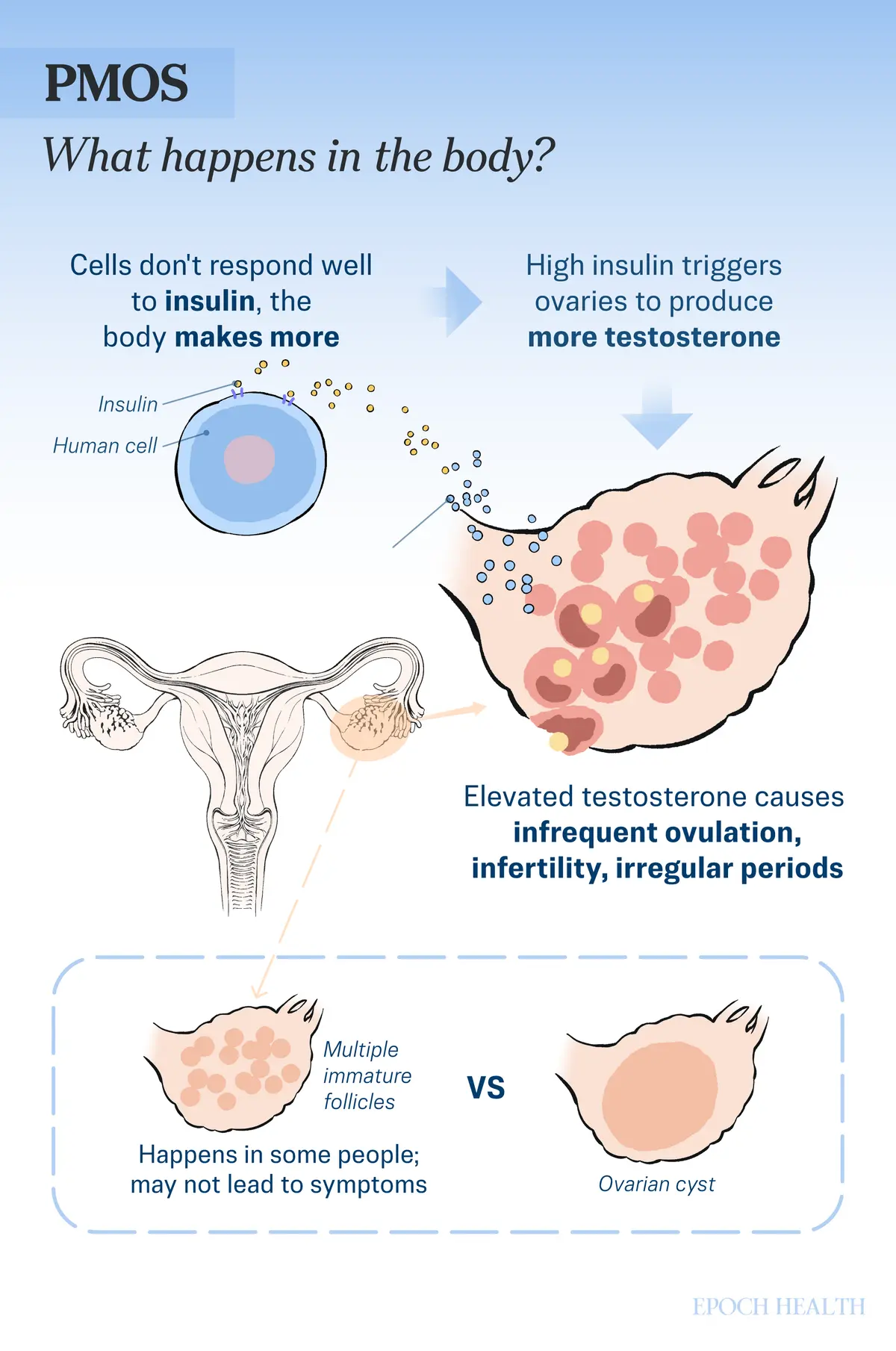
Some women with PMOS have ovaries that appear enlarged or contain an accumulation of small, immature follicles on ultrasound. These small follicles rarely cause symptoms and differ from the large ovarian cysts that people commonly associate with the term “cyst.” The previous name, PCOS, focused heavily on ovarian “cysts,” which led to a narrow focus on the ovaries and contributed to missed diagnoses.
The misleading name reflected a long-standing problem: PMOS has never had a single clear cause. However, it is increasingly thought to involve a combination of different factors, including:
Genetics: PMOS often runs in families, and research suggests that genetic factors are estimated to account for roughly 70 percent of cases. Multiple genes involved in hormone production and androgen regulation have been linked to increased risk.
Insulin Resistance: Approximately 85 percent of women with PMOS have insulin resistance. When the body’s tissues don’t respond effectively to insulin, the body produces extra insulin. High insulin levels can trigger the ovaries to produce excess testosterone, disrupting ovulation and creating a cycle of hormonal imbalance.
Hormonal Imbalance: In PMOS, hormonal imbalances typically involve elevated testosterone (which drives excess hair growth, acne, and irregular periods), elevated luteinizing hormone (which disrupts ovarian function and androgen production), lower levels of sex hormone-binding globulin (leaving more testosterone active in the body), and, in some people, reduced estrogen. Together, these imbalances can compound menstrual and reproductive irregularities.
What Are the Symptoms of PMOS?


PMOS primarily affects girls and women of reproductive age. Symptoms vary widely and may change over time. Some women may have no symptoms at all. Common symptoms include:
Menstruation and Ovulation Irregularities: Hormonal imbalances involving elevated androgen and insulin levels disrupt normal menstrual cycles, causing periods that are irregular, infrequent, unusually heavy or light, or absent altogether. Ovulation may occur irregularly or not at all, which can contribute to infertility.
Excess Hair Growth (Hirsutism): Elevated androgen levels can cause excessive, coarse hair growth on the face and body.
Acne and Oily Skin: Hormonal imbalances can trigger acne and seborrhea (excess oil production).
Skin Tags and Dark Patches: Benign skin tags and hyperpigmentation, typically on the neck or underarms, may appear.
Weight Gain and Obesity: These are common in women with PMOS and can worsen other symptoms.
Hair Thinning or Loss: PMOS can cause male-pattern scalp hair loss because higher androgen hormone levels can shrink hair follicles on the scalp, leading to thinning at the front and top of the head.
Hyperlipidemia (High Blood Fats): Abnormal cholesterol and triglyceride levels can increase cardiovascular risk.
Emotional Difficulties: Anxiety and depression are common in women with PMOS.
Other Symptoms: These include pelvic pain, fatigue, headaches, and sleep problems.
PMOS can present in different forms, known as phenotypes (patterns of symptoms), based on which combination of symptoms and clinical features a person has. These variations explain the wide range of symptom types and severities observed among people with PMOS.
How Is PMOS Diagnosed?
Despite PMOS’s high prevalence, up to 70 percent of women with the condition worldwide are thought to remain undiagnosed, partly because it shares symptoms with many other conditions, including thyroid disease (hypothyroidism), late-onset congenital adrenal hyperplasia (a genetic condition that affects adrenal hormone production), and ovarian cancer.
Your doctor will start by taking a thorough medical and menstrual history, including signs of hyperandrogenism, followed by a physical exam, which may include a pelvic exam. Additional tests may include:
Blood Tests: These may assess hormone levels, including estrogen, FSH, LH, testosterone, and progesterone; metabolic markers (fasting glucose and lipid levels); and rule out other possible causes of symptoms, such as pregnancy. They may include a pregnancy test, prolactin levels, and thyroid function tests. The fasting glucose test can evaluate insulin resistance.
Physicians may screen for cholesterol and hemoglobin A1c to assess the long-term effects of insulin resistance.
Fasting insulin or an oral glucose tolerance test can also be requested to detect insulin resistance earlier, before it progresses to Type 2 diabetes, although these tests are not part of the current diagnostic criteria.
Ultrasound: Transvaginal ultrasound assesses the ovaries’ appearance and structure and provides more accurate results for diagnosing PMOS than other ultrasound methods. In cases where a precise ovarian ultrasound is not available, measuring AMH levels may also help support the diagnosis. AMH is a hormone produced by the small, developing follicles in the ovaries, and its level in the blood mainly reflects the number of remaining follicles (ovarian reserve).
MRI: MRI is not routinely used in the evaluation of PMOS, but pelvic MRI can demonstrate similar features to ultrasound, including multiple small ovarian follicles.
What Are the Treatments for PMOS?
Because there is no known cure, PMOS treatment focuses on managing symptoms. Treatment is individualized based on age, symptom severity, overall health, and whether pregnancy is desired.
1. Menstrual Irregularities
For women who don’t plan to become pregnant in the future, combined oral contraceptives, including birth control pills, patches, and vaginal rings, are the first-line treatment for menstrual irregularities and hyperandrogenism. Lower-dose ethinyl estradiol formulations are often preferred.
Combined oral contraceptives help manage menstrual irregularities, hirsutism, and acne by reducing LH levels and ovarian androgen production, increasing sex hormone-binding globulin, and, in some cases, directly blocking androgen activity. They are not used for women who plan to become pregnant.
2. Infertility
A combination of lifestyle modifications, medications, and, in some cases, surgery can help women with PMOS achieve pregnancy.
Letrozole: A first-line oral medication for infertility in PMOS. By lowering estrogen production, it increases FSH release and stimulates ovulation. Compared with clomiphene, letrozole is associated with higher rates of ovulation, pregnancy, and live births.
Clomiphene: A selective estrogen receptor modulator (SERM) that blocks estrogen receptors in the hypothalamus, stimulating the hormonal signals needed to trigger ovulation. However, it may have a mild anti-estrogen effect on the uterine lining, which can make implantation slightly less favorable.
Metformin: Originally used for Type 2 diabetes, metformin may help improve ovulation in some women with PMOS, particularly those with insulin resistance or impaired glucose tolerance.
Gonadotropin Injections: Injections containing FSH, sometimes combined with LH, directly stimulate the ovaries to develop mature follicles and trigger ovulation. They are highly effective as a second-line therapy but require close monitoring to reduce the risk of multiple pregnancies and ovarian hyperstimulation syndrome (OHSS).
Laparoscopic Ovarian Surgery: A surgical treatment for women who do not respond to medication, it works by reducing androgen and LH levels while increasing FSH, which helps rebalance hormones and may restore normal ovulation.
Assisted Reproductive Technologies (ART): Intrauterine insemination, in vitro fertilization, and other ART procedures may also be options.
However, letrozole, clomiphene citrate, and gonadotropin injections can carry certain risks, including an increased likelihood of multiple pregnancies (such as twins) and OHSS, a condition that may cause abdominal bloating, pelvic pain, and enlargement of the ovaries.
3. Excess Hair Growth
For women not planning pregnancy, the first-line treatment for hirsutism is low-dose antiandrogenic oral contraceptives, which can reduce male hormone levels and their effects. Spironolactone pills and prescription eflornithine cream may also be used.
Cosmetic treatments, including electrolysis, laser hair removal, bleaching, waxing, or shaving, can be used regardless of pregnancy plans and are generally preferred for women trying to conceive because antiandrogen medications should be avoided during pregnancy.
4. Acne
Antiandrogen medications such as spironolactone may help improve acne associated with PMOS. Severe acne may be treated with isotretinoin.
Women who are trying to become pregnant should avoid isotretinoin, as it can cause severe birth defects.
5. Excess Weight
For patients with PMOS and excess weight, bariatric or metabolic surgery, such as gastric bypass or sleeve gastrectomy, may improve weight loss, menstrual regularity, ovulation, and other metabolic health outcomes.
6. Psychological or Behavioral Considerations
Herbal Medicines
Before trying any of the herbal formulas below, consult your doctor and TCM pracitioners for potential side effects and interactions with other drugs.
Free and Easy Wanderer Powder (Xiao Yao San): This traditional Chinese herbal formula is commonly used to treat gynecological conditions, such as PMOS. Its ingredients include licorice root, Chinese angelica, poria, tree peony bark, white atractylodes rhizome, and bupleurum. A 2023 meta-analysis of nine studies involving 736 women with PMOS found that when used alongside conventional treatment, Xiao Yao San improved reproductive outcomes by increasing ovulation and pregnancy rates. It also reduced insulin-related measures, including fasting insulin and insulin resistance.
Atractylodes-Cyperus Phlegm-Resolving Decoction (Cangfu Daotan Decoction): This classic traditional Chinese medicine formula is composed of white atractylodes rhizome, cyperus, pinellia rhizome, citrus, medicated leaven, bile arisaema, poria, bitter orange, fresh ginger, and licorice root. A 2024 meta-analysis of 25 studies involving 1,845 women with PMOS found that Cangfu Daotan Decoction, when used alongside a conventional drug, achieved higher ovulation and pregnancy rates, reduced ovarian volume, lower androgen levels, and improvements in BMI and symptoms of hyperandrogenism, such as acne and hirsutism.
Angelica and Peony Powder (Danggui Shaoyao Powder): This herbal formula’s ingredients include Chinese angelica, white peony root, Sichuan lovage root, white atractylodes rhizome, poria, and water plantain rhizome. A 2025 study of 98 women with PMOS-related infertility found that modified Danggui Shaoyao Powder combined with acupoint embedding improved reproductive and metabolic outcomes compared with medication alone. The combined treatment increased ovulation and pregnancy rates, improved insulin resistance and blood lipid levels, reduced BMI, acne, hirsutism, and helped normalize ovarian morphology.
What Are the Natural and Lifestyle Approaches to PMOS?
Certain lifestyle modifications are considered first-line treatment for PMOS and can significantly improve symptoms.
1. Dietary Changes
Certain dietary patterns have shown benefits for women with PMOS:
Mediterranean Diet: This diet emphasizes nonstarchy vegetables, fruits, whole grains, lean proteins, healthy fats, and low-fat dairy while limiting saturated fats, processed meats, and refined sugars. Its anti-inflammatory properties may be particularly beneficial for people with PMOS, helping to improve insulin sensitivity, support weight management, regulate metabolic health, and reduce the risk of long-term complications such as Type 2 diabetes and cardiovascular disease.
DASH Diet: Rich in fiber and low-glycemic-index foods, the DASH diet, or Dietary Approaches to Stop Hypertension, may help manage PMOS by addressing key metabolic concerns, including insulin resistance, abdominal fat accumulation, and inflammation. It may support blood sugar control, help reduce insulin and androgen levels, promote weight loss, and improve lipid profiles in women with PMOS.
Pulse-Based Diet: A pulse-based diet is a plant-forward, high-fiber diet that emphasizes pulses, which are the edible dried seeds of legumes. A 2020 study involving 30 women with PMOS found that a diet rich in pulses, including lentils, beans, chickpeas, and split peas, was associated with fewer ovarian follicles, reduced ovarian size, lower androgen levels, and more regular menstrual cycles.
Ketogenic Diet: The keto diet is a high-fat, very low-carbohydrate eating pattern that promotes ketosis—a metabolic state in which the body uses fat as its primary fuel source instead of carbohydrates. A 2023 study found that short-term adherence to a keto diet may improve several PMOS-related hormonal and metabolic markers.
Carnivore Diet: As this diet eliminates nearly all carbohydrates, it may improve insulin sensitivity and reduce insulin-driven androgen production. Some women report weight loss, reduced inflammation, improved skin, and better symptom control, but scientific evidence is limited, and the diet carries risks of nutrient deficiencies and increased cardiovascular risk.
Foods to avoid include fried foods, processed meats, and highly processed snack foods, as well as high-sugar cereals and refined flour products. It is also recommended to limit sugary beverages such as sodas, sweetened teas, and sports drinks, as well as alcoholic drinks, as these can contribute to blood sugar spikes, inflammation, and overall metabolic imbalance.
2. Nutritional Supplements
Some supplements may interact with medications. Always consult your healthcare provider to discuss potential drug interactions and possible side effects.
Chasteberry (Vitex): Its fruit contains several bioactive compounds, including monoterpenoids, labdane diterpenoids, and flavonoids, which may help reduce prolactin levels, a hormone that affects reproductive function. Through its hormonal effects, chasteberry may help reduce ovarian cyst formation and improve hormonal balance. A study published in January involving 60 women with PMOS found that daily supplementation with a chasteberry extract significantly improved antioxidant and oxidative stress markers, insulin resistance, cholesterol levels, menstrual frequency, and hirsutism compared with a placebo. There were also reductions in fasting blood sugar, LDL cholesterol, liver enzyme ALT, and ovarian volume.
Inositol: This naturally occurring sugar alcohol is found in fruits, beans, grains, and nuts. A 2023 systematic review of 26 studies involving nearly 1,700 women found inositol to be an effective alternative to metformin for managing PMOS. A 2024 meta-analysis also found it may reduce the risk of ovarian hyperstimulation syndrome during fertility treatment, with fewer side effects than metformin.
Omega-3 Fatty Acids: Research suggests that omega-3 supplementation may help improve several components of metabolic syndrome in women with PMOS, including blood lipids and inflammation, and may support overall metabolic health.
Berberine: This bioactive alkaloid is a natural plant compound found in barberry and Oregon grape. A 2024 meta-analysis of 10 studies involving more than 700 women with PMOS found that berberine, when used with standard medical treatment, increased endometrial thickness, improved ovulation rates, and nearly doubled clinical pregnancy rates, while helping reduce LH and total testosterone levels.
Vitamin D: About 58 percent of women with PMOS are vitamin D deficient, which can worsen insulin resistance, irregular ovulation and menstrual cycles, infertility, and increased cardiovascular risk. A meta-analysis published in January found that vitamin D supplementation modestly improved insulin resistance, reduced inflammation, and lowered testosterone levels compared with placebo.
Curcumin: In a 2021 study involving 72 women with PMOS, participants who took 500 milligrams of curcumin three times daily experienced significant reductions in fasting blood glucose and dehydroepiandrosterone levels compared with those receiving a placebo, suggesting benefits for metabolic and hormonal aspects of PMOS.
3. Exercise and Physical Therapy
Exercise is considered a first-line treatment for PMOS, particularly in overweight and obese PMOS women and adolescents.
4. Tai Chi
5. Yoga
6. Mindfulness-Based Stress Reduction (MBSR)
Many women with PMOS experience psychological difficulties such as depression. MBSR, including meditation practices, has been shown to reduce emotional symptoms such as anxiety and stress, as well as improve physical symptoms such as pain. In addition, MBSR may help lower blood pressure, blood glucose, and inflammation by improving autonomic nervous system regulation, potentially reducing the risk of diabetes and cardiovascular disease in people with PMOS.
How Does Mindset Affect PMOS?
Although mindset does not cause PMOS, it can significantly influence how its symptoms are managed and the patients’ quality of life.
PMOS is associated with higher rates of stress, anxiety, depression, and reduced quality of life, partly due to hormonal changes and partly due to the effects of symptoms such as infertility and undesired changes in physical appearance, including weight changes, acne, and excessive hair growth.
A positive and adaptive mindset can encourage stress management and coping strategies that may help reduce perceived symptom severity and improve adherence to lifestyle changes, which may indirectly affect hormonal balance and symptoms.
How Can I Prevent PMOS?
There is currently no known way to prevent PMOS in most people, although early detection and management of insulin resistance may help reduce risk in the future.
Risk can potentially be lowered by maintaining a healthy weight, eating a balanced diet, exercising regularly (at least 30 minutes, three times per week), eating meals consistently (including breakfast), and avoiding smoking and excessive alcohol intake.
Because women with PMOS can develop a wide range of complications, close follow-ups are highly recommended.
What Are the Possible Complications of PMOS?
Because PMOS affects multiple body systems, possible complications over time include:
Metabolic and Blood Sugar-Related Conditions: These include an increased risk of insulin resistance, prediabetes, Type 2 diabetes, gestational diabetes (blood sugar levels rising during pregnancy), metabolic syndrome, obesity-related complications, and nonalcoholic fatty liver disease.
Increased Cardiovascular Risks: Over time, excess male hormones may cause cardiovascular problems, including high blood pressure and elevated LDL cholesterol, as well as a higher long-term risk of cardiovascular disease, such as angina, heart attack, and stroke.
Reproductive and Gynecological Complications: These include subfertility or infertility, sexual health problems, and an increased risk of endometrial hyperplasia (thickening of the uterine lining) and uterine cancer due to hormonal imbalance and irregular menstruation. Although many women with PMOS are able to conceive, they may face an increased risk of pregnancy-related complications, including gestational diabetes, preterm birth, and preeclampsia (new-onset high blood pressure and signs of organ damage during pregnancy).
Mental Health Problems: These include higher rates of anxiety, depression, eating disorders, and other related conditions.
Skin Conditions: Excess androgens commonly cause dermatologic complications such as hirsutism and severe acne by stimulating hair follicles and sebaceous glands.