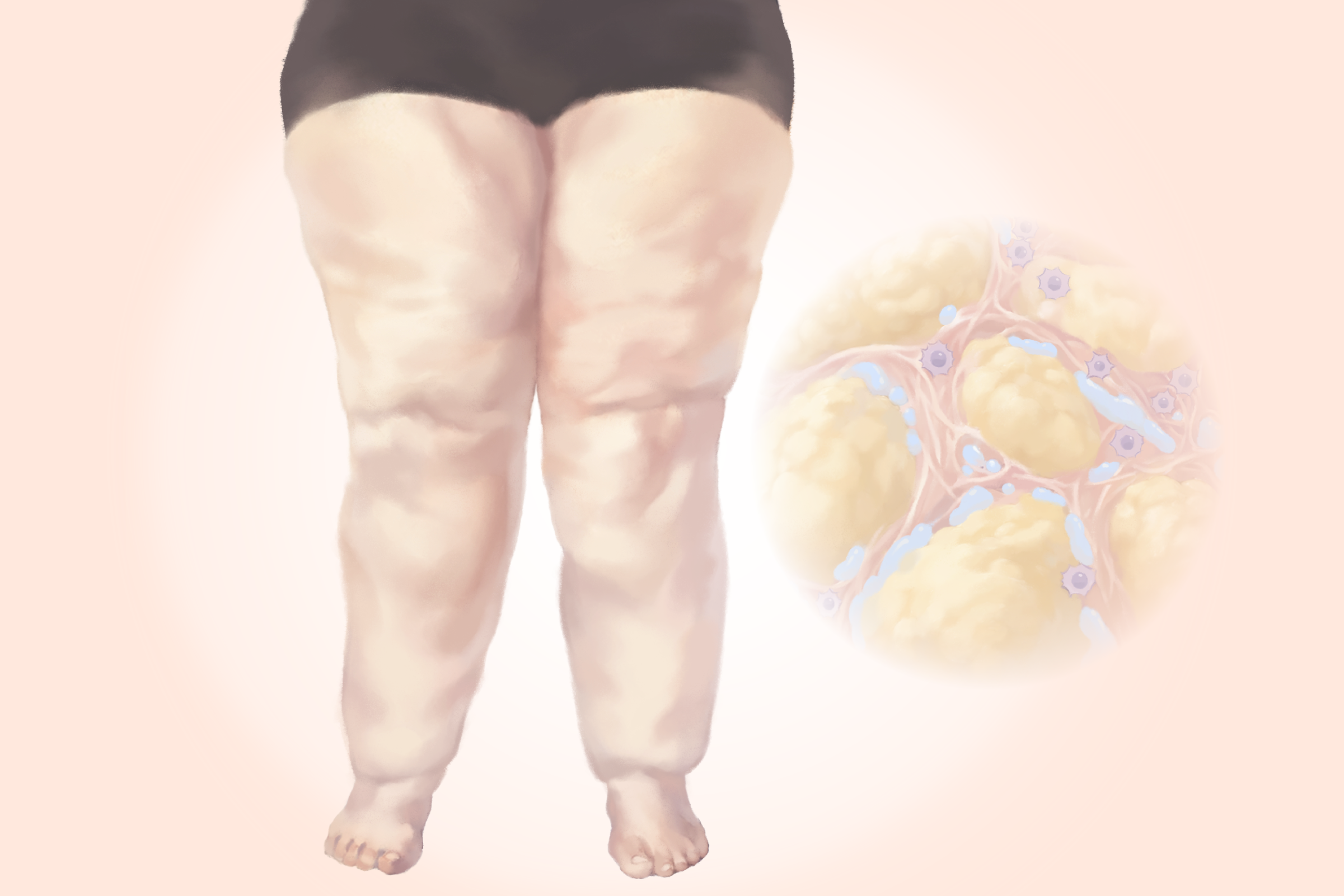
Lipedema is a chronic condition that causes painful fat accumulation, primarily in the legs. It affects an estimated 11 percent of women and is rare in men.
Unlike ordinary body fat, lipedema fat resists ordinary diet and exercise. Making matters worse, the condition is underdiagnosed and often mistaken for obesity or other conditions, leading to a 10- to 15- year delay in diagnosis. During that time, symptoms often worsen, and people may undergo unnecessary treatments for the wrong condition.
What Are the Symptoms of Lipedema?
Lipedema, also known as lipoedema, is derived from the Greek words for fat (“lipos”) and swelling (“edema”). The first symptoms often occur before age 30.


The most recognizable feature of lipedema is disproportionate, symmetrical fat buildup in the limbs—most commonly the legs. In about 30 percent of cases, the upper arms are also affected. The German S2k guideline states that lipedema occurs only in the legs and/or arms, whereas other sources also include the buttocks, hips, and, less commonly, the abdomen. This lack of a clear definition contributes to inconsistent recognition and diagnostic delays.
Affected limbs often appear column-like, with distinct cuffs at the ankles or wrists where the abnormal fat stops, and the hands and feet remain unaffected.
Lipedema fat also feels different from regular body fat. It is firmer and often nodular or lumpy beneath the skin.
Symptoms typically worsen over the course of the day and may include:
Tenderness to touch and mild to severe pain, including neuropathic pain (burning, tingling, or numbness)
A feeling of heaviness or pressure in the legs, especially after prolonged standing
Swelling that does not improve with leg elevation and usually leaves no indentations when pressed
Easy bruising
Spider veins (telangiectasias)
Fatigue and muscle weakness
Cold skin
Flat feet or fallen arches
Joint hypermobility (unusually flexible joints)
What Causes Lipedema?
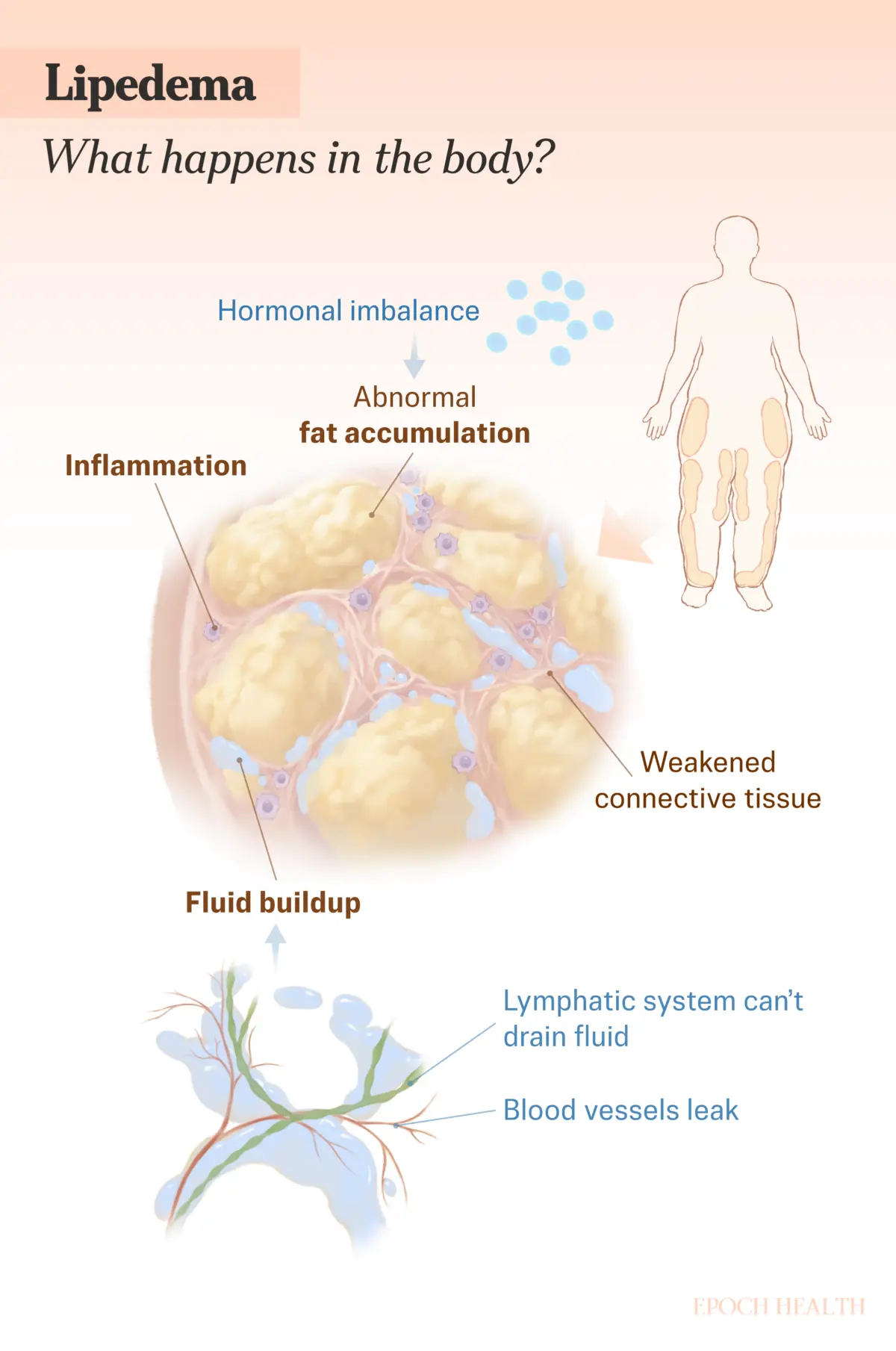
Lipedema is not caused by overeating or lack of exercise. Its exact cause is still unknown and likely varies from person to person. Current evidence suggests a combination of genetic predisposition, hormonal and metabolic influences, connective tissue abnormalities, and dysfunction of the small blood vessels and lymphatic system.
Genetics
Lipedema often runs in families, with 60 percent to 80 percent of people reporting affected family members. Several genes have been associated with lipedema, although not everyone with these genetic variants develops the condition, as differences in gene expression and environmental factors also play a role.
Hormonal Triggers
Lipedema often develops or worsens during periods of hormonal change, including puberty, pregnancy, and menopause, suggesting that sex hormones—particularly estrogen and progesterone—play a central role. Current evidence indicates these hormones may promote lipedema by altering how fat cells grow and store fat, and by influencing local inflammation and microvascular function in the affected tissue.
Emerging research points to broader hormonal imbalances and metabolic disruptions involving leptin and other fat-tissue signaling molecules. Together, these hormonal and metabolic changes may contribute to abnormal fat accumulation.
Obesity can worsen swelling while increasing stress on the lymphatic system. In men, lipedema is rare and is usually associated with severe liver disease, elevated estrogen with low testosterone, or hormone therapy for prostate cancer.
Lipedema may also be triggered by stressful lifestyle changes, surgery, or trauma, likely through associated hormonal disruptions such as elevated cortisol levels.
Connective Tissue Changes
Lipedema is increasingly recognized as a loose connective tissue disorder in which the structural framework supporting fat cells, blood vessels, and lymphatic vessels becomes weakened or disorganized. Changes in the extracellular matrix—the network of proteins that normally provides strength and elasticity to tissues—may contribute to tissue firmness, skin nodules, and joint hypermobility. These connective tissue changes may also weaken blood vessels.
Blood Vessel Dysfunction
Small blood vessels within affected tissue become dilated and fragile, leaking fluid and proteins into the surrounding tissue. This contributes to swelling and the easy bruising commonly seen in lipedema.
Lymphatic Involvement
The lymphatic system normally helps clear excess fluid and waste from tissues, but structural abnormalities in lipedema may contribute to fluid buildup and swelling. Researchers increasingly believe these lymphatic changes may be part of the underlying disease process, not just a later complication. They may also help explain why the affected areas feel heavy and why swelling doesn’t improve with leg elevation.
Emerging Research: Gut Health
Increased intestinal permeability (commonly referred to as “leaky gut”) allows bacterial toxins such as lipopolysaccharide to enter the bloodstream and promote low-grade inflammation. During pregnancy, permeability increases to help support fetal development.
One group of researchers has proposed that these bacterial toxins may accumulate in lower-body fat, contributing to inflammation, abnormal fat growth, and vascular changes.
What Are the Types of Lipedema?
Lipedema is categorized both by where the abnormal fat distribution occurs and by how far the condition has progressed.
The five types describe the pattern of fat distribution:
Type I: Fat extends from just below the waist to the upper thighs (“saddlebag” area).
Type II: Fat extends to the knees, with fat pads on the inner knees.
Type III: Fat extends from the hips to the ankles.
Type IV: Fat involves the arms.
Type V: Fat is limited to the lower legs below the knees.
How Is Lipedema Diagnosed?
There is no single laboratory test or imaging study that can diagnose lipedema. Diagnosis is based on clinical evaluation that considers personal and family history, characteristic physical signs, symptoms, and coexisting conditions such as hypermobility or vascular disease.
Lipedema shares characteristics with several other conditions. Accurate diagnosis requires distinguishing it from lymphedema (fluid buildup due to lymphatic damage), obesity, and venous insufficiency (poor blood return from legs)—all common misdiagnoses that may also occur alongside lipedema.
Laboratory tests are primarily used to rule out organ dysfunction, hormonal disturbances, or medications that can cause fluid retention–including beta blockers, gabapentin, and oral corticosteroids.
To differentiate lipedema from lymphedema, clinicians use specific physical signs, such as the Stemmer sign, which is the inability to pinch a fold of skin at the base of the second toe. This sign is typically positive in lymphedema but negative in lipedema.
The following table compares these and other key characteristics that help differentiate lipedema from the commonly confused conditions.

Imaging is not required for diagnosis, but ultrasound, CT, or MRI scans may be used to rule out other conditions and to study the affected tissue.
Dual-energy X-ray absorptiometry may be used to assess body composition by measuring fat mass and lean body mass, helping distinguish it from general obesity, in which fat distribution is more proportional throughout the body.
Functional Medicine
Beyond standard diagnosis, a functional medicine approach looks for underlying imbalances that may worsen pain, swelling, inflammation, tissue changes, or progression. These may include hormonal shifts, cortisol dysregulation, leptin resistance, metabolic dysfunction, inflammation, thyroid imbalance, and nutrient deficiencies.
Potential laboratory testing may include:
Comprehensive hormone testing
Metabolic markers, such as fasting insulin, HbA1c, and an advanced lipid panel
Inflammatory markers, such as hs-CRP and homocysteine
Nutrient assessment, including vitamin D, magnesium, selenium, and the omega-3 index
What Are the Treatments for Lipedema?
No cure or medication specifically approved for lipedema currently exists. However, an accurate diagnosis ensures appropriate treatment is available to help reduce pain, inflammation, swelling, and disease progression while improving mobility.
Treatment should be individualized and often involves a multidisciplinary team that may include a lipedema specialist, a vascular medicine specialist, an endocrinologist, a physical therapist, a nutrition professional, a dermatologist, and a mental health professional.
Nonsurgical Treatment
Conservative treatment involves treating underlying conditions, providing education on self-management, and using nonsurgical approaches. Case reports show that consistent conservative treatment can reduce symptoms and limb volume and slow disease progression.
Key approaches include the following:
Follow an anti-inflammatory eating pattern
Exercise, especially water-based exercises, and physical or occupational therapy
Receive manual lymphatic drainage
Wear customized compression stockings or bandages, when tolerated; these are contraindicated in people with peripheral arterial disease
Undergo complex decongestive therapy (manual lymphatic drainage followed by compression wrapping)
Use sequential compression devices (such as recovery boots)
Practice good skincare (gentle cleansing, careful drying, and regular moisturizing) to protect the skin barrier and reduce infection risk
Medications
No medications are FDA-approved specifically for lipedema. However, the following may be used in certain cases:
Metformin is used when metabolic complications are present
Weight-loss medications, including GLP-1 receptor agonists, when obesity coexists with lipedema; however, these medications are not FDA-approved for lipedema and have not been shown to selectively reduce fibrotic lipedema fat
Sympathomimetic amines (amphetamine, dextroamphetamine, or phentermine), which showed promise in reducing weight, body size, swelling, and pain while improving quality of life
According to lipedema guidelines, the following medications should be avoided because they may worsen symptoms by promoting fluid retention or weight gain:
Diuretics
Medications that promote weight gain, such as some antidepressants, antipsychotics, diabetes medications, and systemic steroids
Thiazolidinediones (a type of diabetes medication)
Medications that increase edema, such as certain calcium channel blockers, including amlodipine
Counseling
Some researchers believe the psychological stress of lipedema may be more severe than the physiological stress. Often, women with lipedema are told their fat and symptoms are caused by overeating and inactivity. This misunderstanding can contribute to disordered eating, “fat shaming,” anxiety, depression, and social isolation. Consequently, counseling can be an important part of treatment.
Surgical Options
Surgery is not a first-line treatment and does not replace conservative care. Options include:
Liposuction
Although no randomized controlled trials have yet evaluated liposuction for lipedema, some nonrandomized studies report reduced symptoms and slowing of progression, particularly in the early stages. A specialized technique, known as tumescent liposuction, is considered the most effective surgical treatment and involves infusing local anesthetic and epinephrine into the fat to make tissues firm (“tumescent”) and easier to remove. A follow-up procedure may be necessary to remove remaining sagging tissue. It is important that both procedures conserve the lymph vessels and are performed by a surgeon experienced in treating lipedema. Continued conservative treatment is still required after surgery.
Bariatric Surgery
In cases where obesity coexists with lipedema, bariatric surgery may be considered to improve mobility and metabolic health. Studies show that patients can lose substantial weight and experience reductions in leg volume, but many continue to experience lipedema-related symptoms, including pain and swelling. The potential risks, complications, and recovery time of each procedure should be carefully considered.
Lymphatic Surgery
In rare, advanced cases with significant lymphedema, specialized lymphatic surgery may be combined with debulking procedures, but these are typically reserved for complex cases at expert centers.
Bioidentical Hormone Replacement Therapy
Some functional and integrative clinicians use bioidentical hormone replacement therapy as an adjunctive therapy when hormone imbalances may be contributing to symptoms.
Treating Comorbid and Related Conditions
Because lipedema often occurs with other conditions such as thyroid dysfunction, insulin resistance, fibromyalgia, and Ehlers-Danlos syndrome, comprehensive treatment should address all contributing factors.
What Are the Natural and Lifestyle Approaches to Lipedema?
Daily habits—including diet, hydration, supplements, gut support, and exercise—may help reduce pain and swelling and increase energy.
Adequate Protein
Adequate protein intake is important for preserving muscle mass and supporting mobility, particularly during weight loss. Quality protein sources include free-range poultry, grass-fed and finished beef, wild-caught omega-3-rich fish such as salmon, sardines, and mackerel, eggs, and organic legumes such as lentils, chickpeas, and beans when tolerated.
Weight loss can improve pain and quality of life. Recent studies challenge the idea that lipedema fat is completely resistant to diet-induced weight loss, particularly in people with both obesity and lipedema. Even a 3 percent reduction in body weight has been associated with a significant decrease in leg fat mass.
Beyond body weight and muscle health, what and how you eat can also influence inflammation and tissue health in lipedema.
Anti-Inflammatory Nutrition
Although research on dietary interventions for lipedema remains limited, anti-inflammatory approaches are consistently recommended because inflammation appears to play a role in tissue dysfunction and pain.
A whole-food, anti-inflammatory eating pattern emphasizes colorful fruits and vegetables rich in antioxidants and polyphenols, along with herbs and spices such as turmeric, ginger, garlic, and onion. Healthy fats from extra virgin olive oil, avocados, walnuts, almonds, chia seeds, and flax seeds may also help reduce inflammation.
Reducing refined carbohydrates, added sugars, ultra-processed foods, and excess sodium may further help reduce inflammation and swelling. Gluten or other foods can also trigger inflammation or fluid retention in some people.
Alcohol should be minimized, as it can impair lymphatic function and contribute to inflammation.
Structured Dietary Approaches
Some people may benefit from a more structured anti-inflammatory diet. Small studies suggest ketogenic and low-carbohydrate diets, including Mediterranean-style ketogenic variations, may improve weight management, pain, and quality of life in some people with lipedema. For example, a modified Mediterranean diet has been associated with improvements in body composition, while a Mediterranean-style ketogenic diet was linked to reductions in inflammation markers, body weight, fat, and leg circumference over seven months.
Anyone following a very low-calorie ketogenic diet should work with a nutrition professional to ensure adequate vitamin and mineral intake and to transition to healthy eating habits for long-term maintenance.
Supporting Gut Health
Research links gut microbiome imbalances and increased intestinal permeability to chronic low-grade inflammation, a key driver of lipedema symptoms. While direct studies on gut health interventions in lipedema are lacking, supporting gut barrier integrity and microbial balance may help reduce systemic inflammation. Strategies include:
Prebiotic Foods: Fiber-rich foods such as garlic, onions, leeks, asparagus, Jerusalem artichokes, and green bananas feed beneficial gut bacteria and support microbial diversity.
Glutamine: Supports intestinal lining integrity and may help reduce permeability
Fermented Foods: Yogurt, kefir, raw sauerkraut, and kimchi provide beneficial probiotics that support microbiome balance
Because gut microbiome imbalances vary significantly between people, comprehensive stool analysis and targeted protocols are best implemented with guidance from a knowledgeable practitioner.
Hydration
Adequate hydration supports circulation and lymphatic flow. General recommendations suggest a total daily fluid intake of 3.7 liters for men and 2.7 liters for women, including fluids from food and beverages. Water and other unsweetened beverages should provide most of the fluid intake. Fluid needs increase with exercise, heat exposure, and sweating.
Supplements
The effectiveness of dietary supplements has not been widely studied for lipedema specifically. However, several micronutrients and bioactive compounds have evidence supporting anti-inflammatory, antioxidant, vascular, or lymphatic effects that may be relevant to lipedema symptoms. These include omega-3 fatty acids, vitamins B12 (methylcobalamin or hydroxycobalamin), C, and D, diosmin and hesperidin, N-acetylcysteine, quercetin, selenium, curcumin, bromelain, and serratiopeptidase
Nutrient testing before supplementing is recommended. Because individual needs, tolerances, and genetic variations affect how supplements are absorbed and used, working with a knowledgeable professional is recommended to ensure supplementation is safe, targeted, and appropriate.
Exercise and Lymphatic Support
Low-impact exercise, particularly water-based exercise and exercises that activate the calf muscles, offers both physical and mental benefits. It can improve mobility, reduce joint stress, and support healthy lymph flow, which is important for preventing progression to lymphedema.
Unlike the cardiovascular system, which relies on the heart as a central pump, the lymphatic system depends on muscle contractions, breathing, and body movement to move fluid through one-way valves.
Evidence-based approaches to support lymphatic flow and drainage include:
Large Muscle Exercise: Walking, marching, dancing, swimming, yoga, and tai chi for at least 10 minutes daily; bicycling at moderate to high intensity three to five times per week
Upper Limb Activation: Arm and resistance exercises, particularly with arm involvement, at least twice daily
Deep, Diaphragmatic Breathing With Muscle Tightening: A combination that creates a pumping action within the lymphatic vessels
Manual Lymphatic Drainage: A specialized gentle massage from a certified therapist
How Does Mindset Affect Lipedema?
For many people, the path to a lipedema diagnosis spans years of being told their condition is a matter of willpower or poor lifestyle choices. Years of dismissal and self-blame can take a real toll—and chronic stress makes it worse. Stress hormones, particularly cortisol, can increase inflammation, which worsens lipedema symptoms.
Exercise, sleep, and counseling can support a positive mindset, but one of the most practical mindset shifts may be redefining what progress looks like. Because lipedema fat often resists diet and exercise, the number on the scale, clothing size, and visible weight loss are poor indicators of improvement. More meaningful progress looks different: less pain, better mobility, improved compression tolerance, and fewer bruises.
Focusing on these markers, practicing self-compassion, and connecting with support groups may improve both treatment compliance and quality of life.
How Can I Prevent Lipedema?
There is no proven way to prevent lipedema. However, because genetics alone do not determine whether the condition develops, lifestyle choices that address factors contributing to development may help reduce risk or delay onset, especially in people with a family history.
Support Healthy Hormone Balance
Although hormones cannot be fully controlled, these strategies may help support hormonal health.
Minimize exposure to endocrine disruptors, including plastics, pesticides, synthetic fragrances, and certain personal care products.
Manage stress through meditation, adequate sleep, and stress-reduction practices to help support healthy cortisol levels.
Maintain a healthy weight, as excess body fat can contribute to estrogen dominance.
Prioritize seven to nine hours of quality sleep to support hormone regulation.
Reduce dietary phytoestrogens if you are sensitive to foods such as soy, flaxseed, and certain legumes.
Optimize Metabolic Health
Supporting metabolic health may help reduce inflammation and improve overall health.
Follow an anti-inflammatory diet.
Maintain stable blood sugar through balanced meals with adequate protein, healthy fats, and a lower-carbohydrate eating pattern.
Consider intermittent fasting or time-restricted eating (under professional guidance) to improve metabolic flexibility.
Support Connective Tissue and Vascular Health
Supporting connective tissue and healthy blood vessels may help maintain tissue integrity and circulation.
Ensure adequate vitamin C, which is essential for collagen synthesis and connective tissue integrity.
Eat foods containing collagen-supporting nutrients, including copper and zinc (nuts, beans, eggs, and fish), silica (leafy greens, whole grains, and beans), and the amino acids glycine, proline, and lysine (chicken, fish, eggs, and legumes).
Stay well-hydrated to support tissue health.
Eat foods rich in bioflavonoids and antioxidants, such as berries, citrus fruits, dark leafy greens, onions, apples, dark beans, and green and black tea, to support capillary strength and reduce vascular fragility.
Consider supplements such as horse chestnut under professional guidance to support vascular health.
Build daily habits that keep lymph moving, such as regular low-impact exercise and deep breathing.
What Are Possible Complications of Lipedema?
Without early diagnosis and treatment, lipedema can lead to a range of physical and psychological complications.
Physical Complications
As lipedema progresses, it can affect multiple body systems and physical function. Potential complications include:
Secondary Lymphedema (Lipolymphedema): A buildup of fluid in the tissues caused by the lymphatic system not draining properly, worsening swelling and tissue changes. Some researchers consider this a fourth stage in the disease progression, while others classify it as a complication.
Mobility Impairment: Progressive fat accumulation and joint stress can limit walking and daily activities.
Orthopedic Problems: Excess weight, joint hypermobility, and muscle weakness may contribute to flat feet, knock knees, swayback, ankle pronation (rolling inward), osteoarthritis, and other joint damage.
Venous Disease: Chronic pressure on veins can lead to venous insufficiency, which may progress to skin discoloration and venous ulcers in severe cases.
Blood Clots (Venous Thromboembolism): Multiple conditions that commonly occur alongside lipedema can increase the risk of blood clots, including deep vein thrombosis and pulmonary embolism.
Bacterial Infections: Cellulitis and erysipelas (skin infections), as well as lymphangitis (infection of lymphatic vessels), are more frequent, especially when lymphedema develops. Symptoms may include red, hot, painful, swollen skin, red streaks extending toward lymph nodes, and fever.
Skin Ulceration: In advanced lipedema, compromised circulation and lymphatic function may lead to nonhealing wounds separate from venous disease.
Psychological and Social Complications
The physical effects of lipedema can also affect emotional well-being and daily life. Potential complications include:
Depression and Anxiety: Years of misdiagnosis, dismissal, and visible body changes can contribute to psychological distress.
Social Isolation: Pain, mobility limitations, and body image concerns may reduce social engagement.
Eating Disorders: Repeated failed weight-loss attempts and body dissatisfaction may increase the risk of disordered eating.
Reduced Quality of Life: The combined physical and emotional toll can significantly affect daily functioning and overall well-being.
Early recognition and comprehensive treatment can slow disease progression and reduce the risk and severity of these complications.




