

Monoclonal antibodies have had their share of ups and downs in the timeline of COVID-19 treatments—but according to news headlines spanning the past two years—not nearly as much as some of the other off-label drugs like ivermectin and hydroxychloroquine. Most of the controversy, if any at all, began at the end of last year, when a handful of preprints written by quite a few scientists said certain brands of monoclonal antibodies would not work for the Omicron variant.
The State of Florida was using sotrovimab—one of the drugs that lost its Emergency Use Authorization (EUA) in January. Meanwhile companies like Eli Lilly (partnered with AbCellera and AstraZeneca) were poised to benefit with exclusive authorizations. The losers for the U.S. monoclonal markets became Regeneron, who makes REGEN-COV, and GlaxoSmithKline (GSK) partnered with Vir Biotechnology—the maker of sotrovimab.
Yet people can still get monoclonal antibodies if they are available in their regions and states, and there are still pharmaceutical companies across the globe whose emergency use permits have not been revoked. Eli Lilly still has one more monoclonal antibody product in the game, and had to add another monoclonal antibody to another for more potency. The company conceded to the FDA’s decision. Regeneron vowed to tweak its formula to make it Omicron-resistant, while GSK/Vir rushed to prove their product indeed works for Omicron, and that the science used to edge out the competition was not clinically valid.
A Different Kind of Treatment
In August of 2021, Florida newspapers reported the opening of monoclonal antibody clinics across the state. The viral photo people saw on the news was a moaning, crying, immobile woman, lying on the floor while waiting in line at a Jacksonville monoclonal antibody site. Without much information to go on, this desperate image has become the poster child of monoclonal antibodies.Nobody wanted to be as sick as that woman on the floor, but at the same time, very few people understood what exactly that treatment was at the end of the line—monoclonal antibodies may be one of the least understood treatments on the market. People know these treatments are experimental, but their mechanisms and origins are certainly not common knowledge.
“Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens, such as viruses like SARS-CoV-2,” as explained by the FDA. They come with especially strange names that can be easily confused with the names of antibiotics and steroids in the wax and wane of COVID-19 treatments and therapies.
It’s a competitive market—and one that relies heavily on the latest science and clinical trials, as well as emergency approval from governments and nations.
If they can find them in their state despite complications and contracts, Americans who are as sick from COVID as the woman on the floor have only two left to choose from: Eli Lilly/AbCellera’s bebtelovimab or AstroZeneca’s Evusheld tixagevimab/cilgavimab.
Products and Partnerships
In the world of monoclonal antibodies, there have been about seven major players:The Variant Shift
When preprints of studies found that existing monoclonal antibodies may not be effective for variants like Omicron, everything changed.Despite that apparent effectiveness, monoclonal antibodies companies were already losing their places on the treatment field.
“Given the latest data showing the Omicron variant of SARS-CoV-2 is responsible for 99 percent of current COVID-19 infections, we are pleased that the FDA is following the scientific evidence and limiting the use of monoclonal antibody treatments to those that are effective against the Omicron variant,” said Harmon.
Florida Disagrees
The announcement was confusing for several reasons: First, states like Florida, which had the most robust monoclonal antibody clinic and hospital program of any state in the United States, had been working from a Standing Order for Regeneron’s REGEN-COV, Eli Lilly’s bamlanivimab and etesevimab combination, and GSK/Vir Biotechnology’s sotrovimab for the treatment and post-exposure prophylactic use for COVID-19.In response to the change, Florida Department of Health released a statement on January 24 that all monoclonal antibody state sites will be closed until further notice.
The Communications office said, “Florida disagrees with the decision that blocks access to any available treatments in the absence of clinical evidence. To date, such clinical evidence has not been provided by the United States Food and Drug Administration (FDA).”
The Florida Department of Health had been correct. There had been no clinical evidence—just pre-prints supported by Zuckerberg’s CZI.
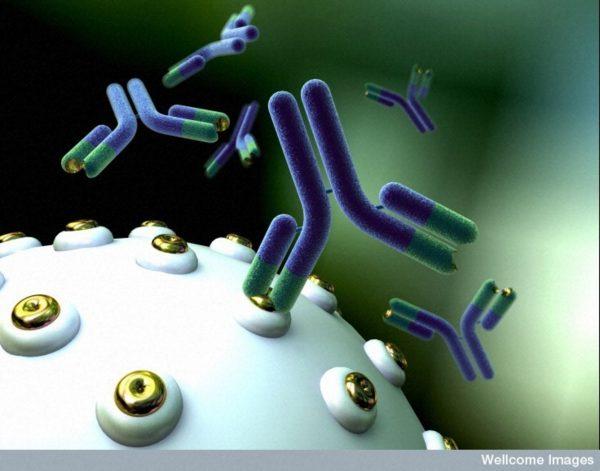
The second reason people were confused is because the average citizen is unclear on what exactly monoclonal antibodies are. Descriptions on the news have been vague. People hear that when a monoclonal antibody is injected into the body, it binds to the spike protein of the SARS-CoV-2, consequently blocking cellular entry and COVID-19 infection.
Basically, the information people are given, is that they make you feel better if you get sick with COVID. You have to get it right away—within the first ten days—and it’s made of antibodies. The antibodies get injected straight into a person’s system and keep the spike protein from entering the cells. Most publications describe monoclonal antibodies as a precision immune booster, a last resort for when you become sick, but not sick enough for the hospital.
The third reason people were confused is because they didn’t know if monoclonal antibodies were safe. People didn’t have the information to know or be convinced that a treatment they hadn’t heard of before the pandemic was safe, and a great many of them had lost trust in their government and institutions offering the treatment.
A Repurposed Drug Treatment
Monoclonal antibodies technology is not new. The treatments have been around for nearly 50 years. The use of monoclonal antibodies in pharmaceuticals began in 1975 at the Laboratory for Molecular Biology in England when researchers developed a way to create cells that could pump out streams of identical antibodies. In the ‘80s, monoclonal antibodies were used in diagnostics for pregnancy tests, and approved in the late ’90s for targeted therapies for a wide range of diseases and disorders, from cancer to psoriasis.Like many treatments during the pandemic, recommendations and approvals came and went depending on many complex factors—and not without controversy.
Promising trials for monoclonal antibodies in the early months of the pandemic led to emergency use authorization (EUA) in the United States for Regenoron’s monoclonal antibodies casirivimab and imdevimab and Eli Lilly/AbCellera’s drug bamlanivimab.
Many other pharmaceutical companies began Phase II and III trials, Vir and GlaxoSmithKline, Brii, Sorento, and AstraZeneca. Initial evidence from Regeneron and Eli Lilly indicated their drugs decreased hospitalizations and medical visits, and reduced viral loads for outpatients in the early stages of disease and worked best in high-risk patients with low native antibody response.
Additional efforts to study potential impact on transmission were underway, and due to the nature of the intravenous formulation, clinical and logistical challenges were analyzed.
Where do Monoclonal Antibodies Come From?
Monoclonal antibodies have been described to the public as a 30-minute injection of purified, laboratory-produced molecules that act as substitute antibodies. To most, this sounds pretty benign, and no one seemed to be sounding the alarm that monoclonal antibodies are unsafe, despite the emergency approvals they’ve relied upon.If you read one of the many articles on monoclonal antibodies, the explanation usually begins with point A: the lab-produced substitute antibody. But the antibody in the IV bag is really point B.
The article states, “Mice are immunized with an antigen and later their blood is screened for antibody production. The antibody-producing splenocytes are then isolated for in vitro hybridoma production.”
Next, the myeloma cells are prepared and after a fusion process, are formed into hybridomas (cultures of hybrid cells). Then the clones are screened and selected on the basis of antigen specificity and immunoglobulin class, characterized, scaled up, weaned off, and finally expanded into desired antibodies.
So after point A, and point B, we have point C: a time of action for the new antibody.
The FDA information site describes point C as the time when the antibodies “may block the virus that causes COVID-19 from attaching to human cells, making it more difficult for the virus to reproduce and cause harm. Monoclonal antibodies may also neutralize a virus.”
Then we have point D, the time after a person ideally recovers. We don’t really know much about point D—or how the immune system will welcome new synthetic antibodies. Due to the treatment being experimental, we don’t have long-term studies to determine exactly what point D looks like. Time will tell, however Dr. Anthony Fauci of the National Allergy and Infectious Diseases endorses the treatment.
Fauci said during a White House briefing in August, 2021, “We recommend strongly that we utilize this to its fullest,” calling monoclonal antibody treatment “effective” yet “underutilized” by most physicians treating the early cases of the virus.
The study explains that Regeneron Pharmaceuticals, the New York-based biotechnology company that produces REGEN-COV monoclonal antibodies for COVID, uses human antibodies obtained from transgenic (organism with artificial DNA from an unrelated organism) human antibody mice, containing “two fully human immunoglobulin G1 (IgG1) antibodies, one selected from the Velocimmune mouse platform and the other isolated from human subjects.”
Whether people have informed consent that their monoclonal antibody treatment involves “genetically humanized mice,” monoclonal antibodies continue to be utilized across the world as an emerging technology.
Support for Monoclonal Antibodies
Prominent figures and heads of state have recovered from COVID-19 with the concurrent use of monoclonal antibodies. President Donald Trump recovered from COVID-19 using several treatments, including monoclonal antibodies, remdesivir, steroids, vitamins, and zinc.Podcaster Joe Rogan recovered from COVID-19 using monoclonal antibodies, ivermectin, Z-pac, steroids, and what he called “the kitchen sink.”
Even as Florida Governor Ron DeSantis expanded the monoclonal antibodies program across the state, not much was written about monoclonal antibodies by the media.
Monoclonal antibodies are challenging to manufacture, time-consuming, and expensive, but DeSantis made these treatments free for his citizens.
At the time, in Florida, the news barely reported that clinics were opened as COVID-19 treatment centers, and many left out the words “monoclonal antibodies” in the headlines. Yet despite little press on the subject, and possibly not the fullest understanding of what the treatment they were getting actually was, Florida citizens flocked to the clinics for treatments.
Prepping the topic, Highwire host Del Bigtree said hydroxychloroquine had become a “political football” and ivermectin is entrenched in battles. Then he asked the big question, “Is there a treatment that anybody likes?” He wondered about that treatment he has heard a little about: monoclonal antibodies.
Bigtree brought on emergency room physician and general practitioner Dr. Richard Bartlett, who was treating patients with Regeneron (casirivimab and imdevimab) monoclonal antibodies in West Texas at the time.
Regeneron’s monoclonal antibodies are the same brand which President Trump received.
“Monoclonal antibodies are not new technology. It’s not something Bill Gates cooked up just the other day,” Bartlett said, after wishing he had treatment access sooner for his patients. He said from “boots on the ground” experience, he’d seen monoclonal antibodies save lives. “This is something that’s real science. What I’m seeing is that in 30 minutes, sitting in a chair—very boring—getting an IV, and their chest pain is going away. Their chest tightness is going away. Their back pain is stopping. The headache, that they’ve had for five days non-stop goes away. They are seeing tremendous results.”
Bartlett said that unlike plasma, monoclonal antibodies have less of a risk of infection because it is a “purified antibody product.” He said he hadn’t seen any adverse reactions in his patients as of the interview.
He asked Bartlett, if these antibodies were designed for the original strain, would they work for future variants?
“The bottom line is I’m seeing great results. We’ve seen articles that it can prevent over 70 percent of hospitalizations and deaths. This is a game changer,” responded Bartlett.
Bartlett mentioned he also found budesonide, a steroid, to be an additional, highly effective co-treatment for COVID-19. He also uses an aspirin a day for his protocol, to prevent blood clots, and antibiotics such as clarithromycin, ivermectin, and supplemental oxygen, depending on each patient’s individual needs.
Problems with Monoclonal Antibodies
According to the Front Line COVID-19 Critical Care Alliance (FLCCC), the guidance approach on monoclonal antibodies by agencies such at the FDA is “complex” and “confusing.”“We are unable to identify a consistent approach to the strength and timing of NIH recommendations and/or updates to the recommendations,” the FLCCC stated in an article on National Institutes of Health (NIH), FDA, and WHO recommendations on monoclonal antibodies, ivermectin, convalescent plasma, remdesivir, anti-IL-6 therapy.
And while monoclonal antibodies have seen their share of revisions in EUA authorizations that confuse professionals wanting to administer alternatives, some say the process has become political.
Kory said, “The reality as to why these medications are ignored and not recommended is quite simple; we live in a healthcare system that is structured to favor novel, highly profitable, pharmaceutically engineered compounds over compounds that have well-established safety profiles, yet little profit to be made … I’ve had a front row seat to the latest battles in that war during COVID-19 and it has been one of the most profound sadnesses of my professional career.”
The American response to COVID-19, led by Dr. Anthony Fauci, director of National Institute of Allergy and Infectious Diseases (NIAID), became the subject of Robert F. Kennedy Jr.’s book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health.”
In a chapter on “mismanaging the pandemic,” Kennedy wrote: “I was struck, during the COVID-19’s early months, that America’s Doctor, apparently preoccupied with his single vaccine solution, did little in the way of telling Americans how to bolster their immune response.”
He continued. “During the centuries that science has fruitlessly sought remedies against coronavirus (aka the common cold), only zinc has repeatedly proven its efficacy in peer-reviewed studies … Yet Anthony Fauci never advised Americans to increase zinc uptake following exposure to infection.”
Doctors have also voiced their concern with the timing of approvals and neutrality of recommendations. Bartlett said the key to the success of monoclonal antibody treatment has been early treatment. “That is what has been ignored, suppressed, and minimized, and censored, is early, effective outpatient treatment,” he said.
Early and effective treatment, outside of the hospital, can take several forms and needn’t be limited to vaccines and costly drugs like monoclonal antibodies. The financial windfall that COVID-19 represented for some interests has raised concerns about the relationship between profit-driven companies, private foundations, and governments.
“Wellcome’s financial interests have been published on the trust’s website and through financial regulatory filings but do not seem to have been disclosed as financial conflicts of interest in the context of Wellcome’s work on covid-19, even as they show that the trust is positioned to potentially gain from the pandemic financially.”
The article explains the Access to COVID-19 Tools (ACT) Accelerator project “hopes to raise billions of dollars and deliver hundreds of millions of treatment courses” during the COVID-19 treatment years, “including dexamethasone and a number of monoclonal antibodies.”
“Revelations of the Wellcome Trust’s financial conflicts of interest follow new reports that another charity, the Gates Foundation, is also positioned to potentially benefit financially from its leading role in the pandemic response,” Schwab writes.
Though efforts from The Wellcome Trust and Bill and Melinda Gates Foundation focused on bringing monoclonal antibodies and vaccines to low- and middle-income nations that had not historically used monoclonal antibodies, many countries were interested in other therapies.
During the pandemic, reports of complementary and alternative medicine (CAM) took a back seat to pharmaceutical products and vaccines, despite the fact many countries were using them to prevent and cure COVID-19.
A survey from the same paper found 22 percent of Saudi Arabians used CAM such as chamomile and garlic to prevent COVID-19. Eighty-percent of the African populations and communities in South America, Europe, and North America used CAM according to the WHO.
The usage of monoclonal antibodies across the globe may take a few new twists and turns, and the questions people may have on whether the treatment is on the good or bad side may need further investigation.



