This copy is for your personal, non-commercial use only. Distribution and use of this material are governed by our Subscriber Agreement and by copyright law. For non-personal use or to order multiple copies, please contact The Epoch Times Reprints.
To prevent cervical cancer, the human papillomavirus (HPV) vaccine has been extensively promoted for young girls and women to protect against high-risk HPV infections that can cause cervical cancer later in life, as an HPV infection is regarded as the main risk factor for cervical cancer.
However, we may be targeting the wrong bull’s-eye. Setting aside the deaths or injuries after HPV vaccination or its potentially harmful adjuvant—all of which we have analyzed based on scientific data and literature in the past three articles in the series—the HPV vaccines themselves are not fundamental to the prevention of cancer. We must instead consider the root causes responsible for HPV infection and cervical cancer.
The Vulnerable Surface of the Cervix
Throughout humanity, the role of a woman has been closely intertwined with marriage and childbirth, impacting her lifelong health and well-being.
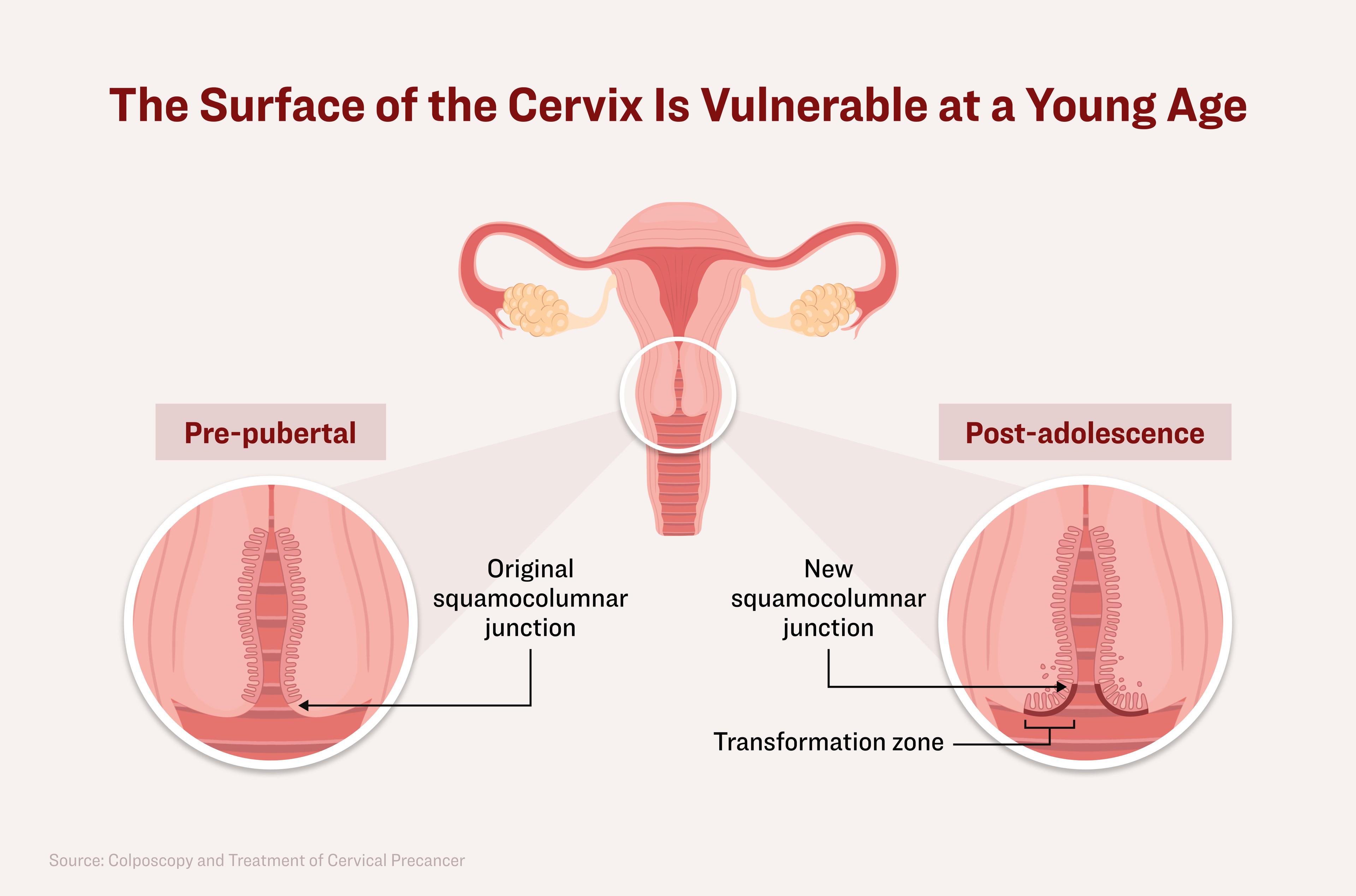
There is a specific area on the surface of the cervix called the “transformation zone“ which is highly susceptible to cervical cancer and often where it originates.
Under the effect of hormones during early puberty, the transformation zone forms and gradually shifts in its location surrounding the cervix area, becoming stronger as a woman matures.
However, at a young age, this zone is not yet well developed or strong enough to defend against viruses and other harmful factors.
At a young age, the transformation zone on the cervix is not well developed enough to defend against harmful pathogens. Illustration by The Epoch Times, Shutterstock
When girls enter puberty, a vulnerable type of cells, known as columnar cells, covers a certain part of the cervix. Only when we mature does another more protective type of cell, called the squamous epithelium, form a layer over the vulnerable columnar cells.
Thus, if sexual behavior occurs during adolescence, this zone will be much more vulnerable to being attacked by a virus, especially the HPV.
Once attacked by the HPV, the protective layers of the cervix’s outer lining will be removed, exposing the underlying layer to the HPV and allowing a precancerous lesion to more easily develop. For young girls who don’t yet have protective layers, it’s even more risky.
Researchers have found that compared with healthy females, young female teens (14 to 19 years old) with precancerous cervical lesions have almost twice the number of columnar cells of the cervix (80 versus 41 percent, respectively), which are less protective barriers to pathogens, suggesting that the biological immaturity of the cervix matters in cancer development.
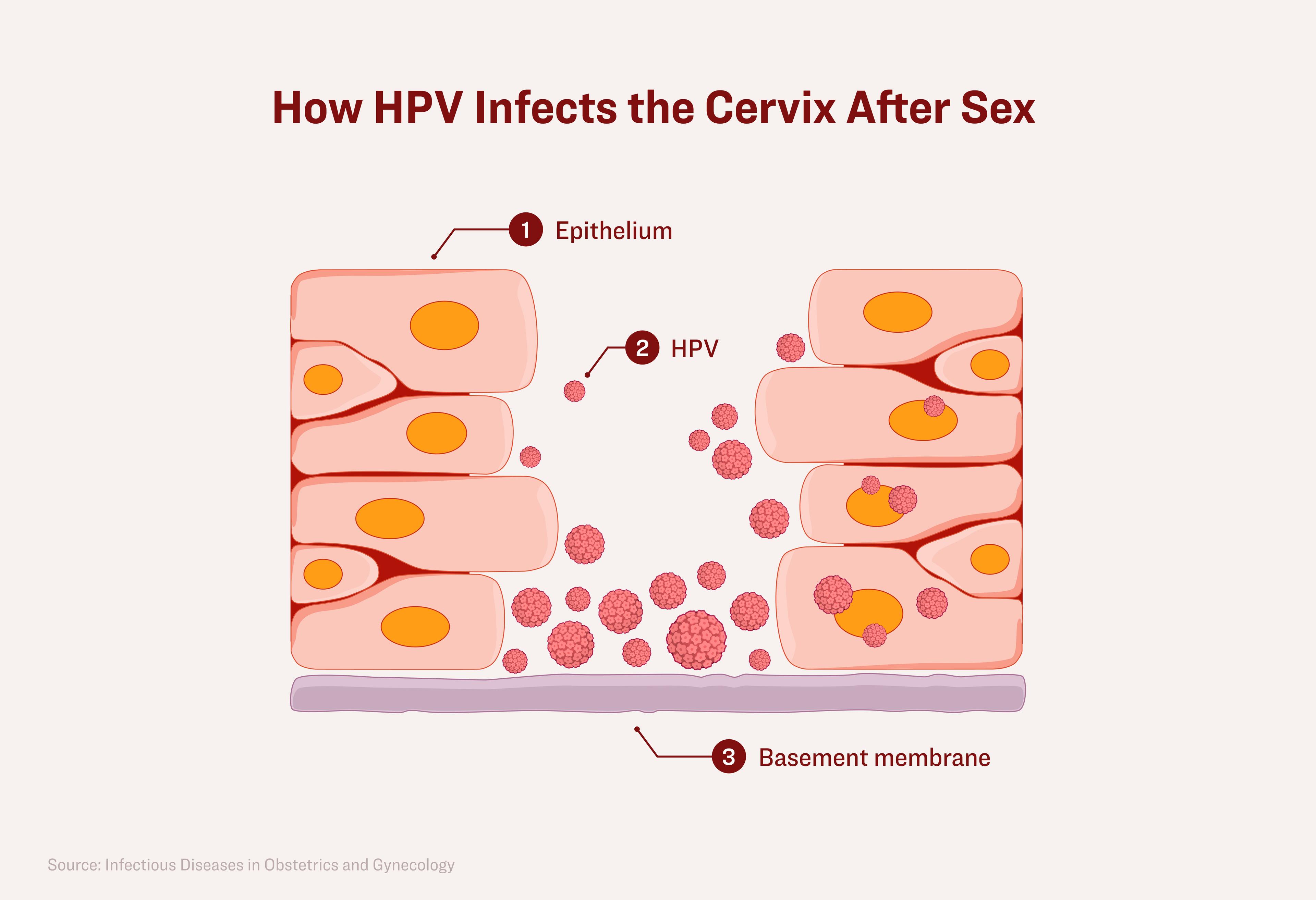
After sex, there are micro-wounds or tiny abrasions to the full-thickness epithelium. These are like cracked tiles on a roof that allow the HPV to pass through and directly bind to the basement membrane, subsequently spreading the HPV and infecting the tiles of the epithelial cells, especially in the transformation zone. It’s important to understand why the maturity of the cervix matters when exposed to an HPV infection.
After sex, there are micro-wounds or tiny abrasions to the full-thickness epithelium. These openings allow HPV to pass through and directly bind to the basement membrane, subsequently spreading the HPV to epithelial cells, especially in the transformation zone. Illustration by The Epoch Times, Shutterstock
A Spanish study revealed that women under the age of 25 were 39 times more likely to engage in sexual activity before the age of 18 than those over the age of 55. This indicates that unhealthy sexual behavior has become more prevalent in younger generations. Similar phenomena have been reported in Brazil.
Therefore, engaging in sexual activity at a young age, having rough sex, or contracting other sexually transmitted infections, can increase the likelihood of HPV entry and infection, thereby increasing the risk of developing cervical cancer during our lifetime.
Age at First Sex Matters
The largest dataset based on a series of multinational case-control etiological studies on cervical cancer was conducted by the International Agency for Research on Cancer (IARC) in France and the Institut Català d'Oncologia in Spain.
An etiological study is a study designed to uncover the cause of a disease.
The analysis included 1,864 cases of invasive cervical carcinoma and 1,719 corresponding controls from developing countries: Morocco, Algeria, Philippines, Thailand, India, Brazil, Colombia, Paraguay, and Peru. Ninety-five percent of the cancer patients and 17 percent of the control group tested positive for HPV DNA. Of those cancer cases, a majority (92 percent), had squamous cell carcinoma.
The most striking finding from this comprehensive analysis was that a woman’s age at first sex has been identified as a strong and consistent factor associated with an increased risk of cervical cancer, regardless of the type of statistical model used for analysis by the investigators.
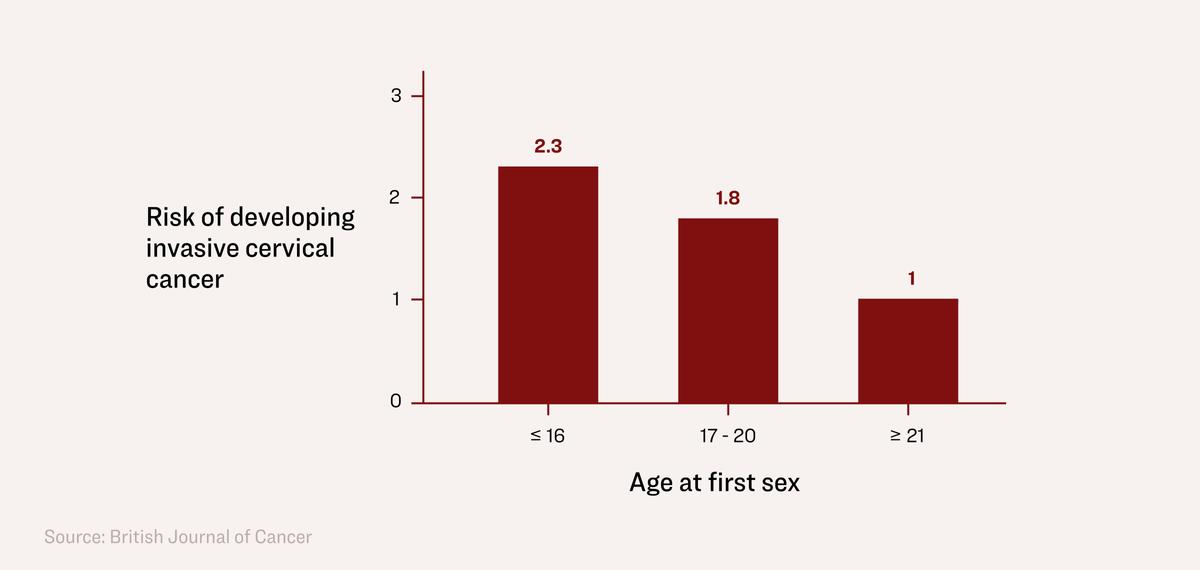
Engaging in sex for the first time on or before age 16 or between 17 to 20 years of age increased the risk of developing invasive cervical cancer by 2.3 and 1.8 times, respectively, compared with women over the age of 21.
Engaging in sex for the first time on or before age 16 or between 17 to 20 years of age increased the risk of developing invasive cervical cancer by 2.3 and 1.8 times, respectively, compared with women over age 21. Illustration by The Epoch Times
The results remained consistent even after the investigators adjusted the model to include the potential confounding factors of HPV infection status, age, country, lifetime number of sexual partners, parity, and education level.
We have explained that the biological maturity of the cervix determines the strength of its protective ability if HPV invades during sexual intercourse. Another factor to consider is that during adolescence, hormonal changes that particularly increase estrogen levels, can lead to acidification of the vaginal cavity, and when the inner cervical lining turns outward, can cause squamous metaplasia—changes in the epithelial cells that can lead to cancer in the presence of HPV.
Number of Sexual Partners Matters
There are three primary reasons that the number of sexual partners matters with cervical cancer.
First, only certain types of HPV strains (e.g., HPV 16 or 18), are linked with cervical cancer and are considered high-risk HPV strains. Having two or more lifetime sex partners is the most important determinant for high-risk HPV infection.
Second, most HPV infection is typically mild and transient, resolving on its own within two years. Only 10 to 20 percent of persistent HPV infections potentially lead to cervical cancer. A greater number of lifetime sexual partners has been associated with reduced clearance rates (35 percent) for an HPV infection.
Third, the number of sexual partners is also a significant risk factor for cervical cancer.
In 1989, researchers at Teen Colposcopy Clinic at the University of California–San Francisco published an epidemiological study of risk factors for precancerous lesions of cervical cancer based on an investigation of 14- to 19-year-old women who visited their clinic.
Compared with the healthy control group of young women without symptoms, those with precancerous lesions (confirmed by either colposcopy or biopsy) had significantly more lifetime sexual partners (8.5 versus 3.1), included a higher percentage of smokers (61 versus 36 percent), and reported higher use of oral contraceptives (61 versus 30 percent).
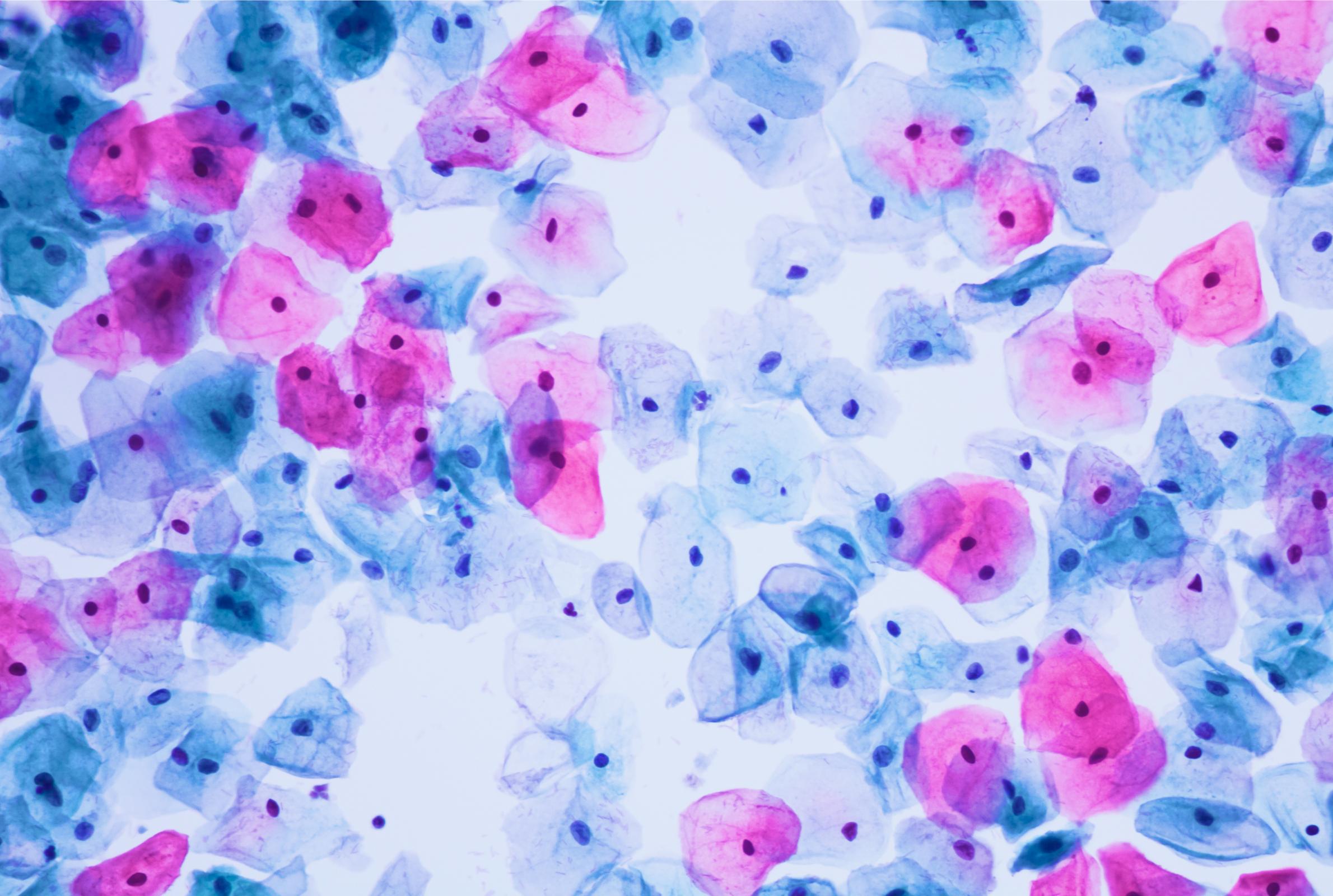
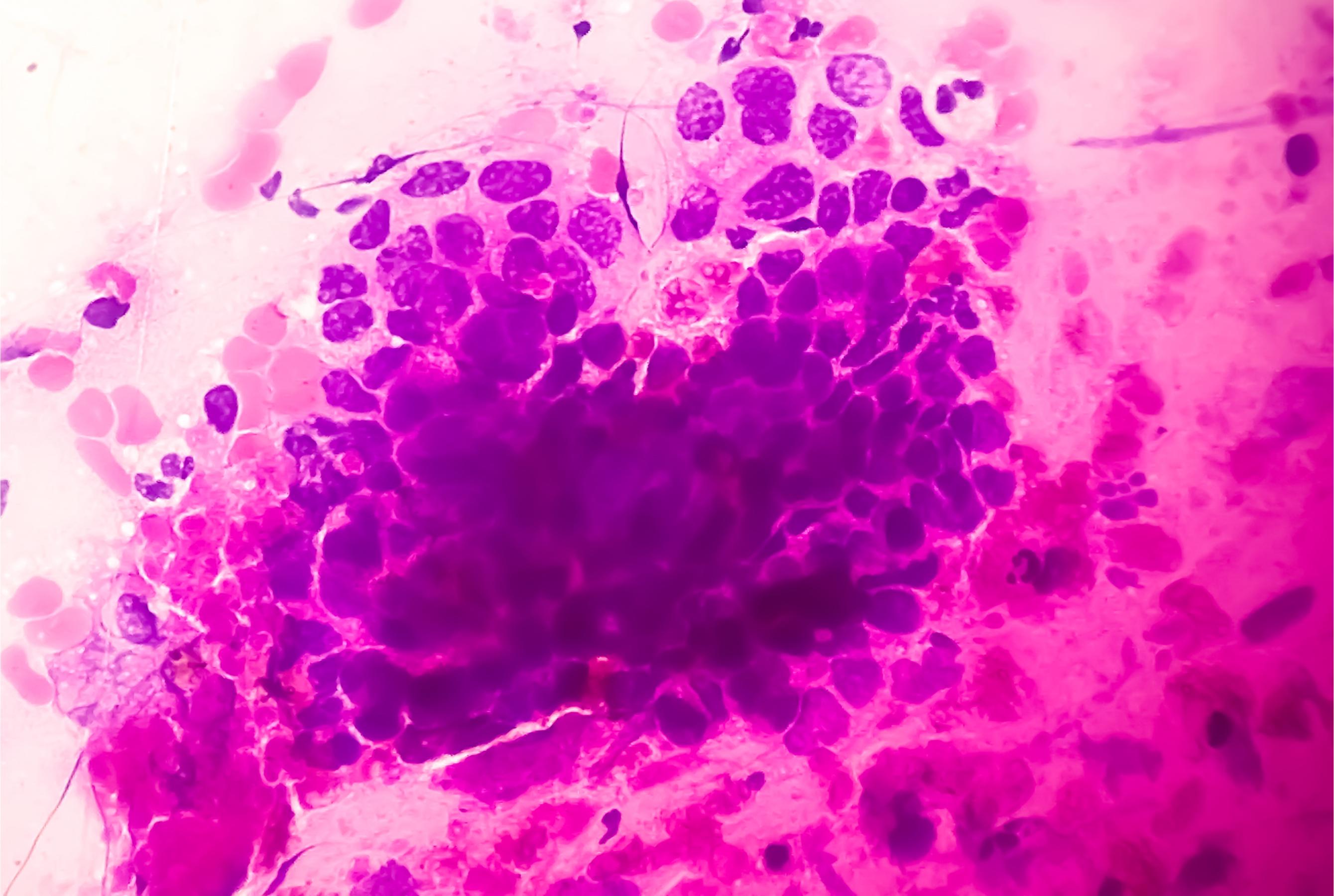
(Left) Normal human cervical squamous epithelial cells from a PAP smear under a lab microscope. (Komsan Loonprom/Shutterstock) (Right) Precancerous high-grade squamous intraepithelial lesion, a sexually transmitted disease associated with HPV, from a PAP smear under a lab microscope (100x zoom). Arif biswas/Shutterstock
A 2020 published Chinese study retrospectively analyzed 549 female patients and found that the more sexual partners one has, the higher the risk of developing HPV-related cancer.
The group with multiple sexual partners consisted of patients who had more than one male sexual partner in the last six months. The non-multiple sexual partners group included patients with the same male partner, those who were not sexually active in the previous six months, and those who occasionally had sex with the same male partner.
The multiple sexual partners group was significantly associated with a positive HPV outcome, including HPV 16 or 18 and other high-risk types of HPV infections. They also had a significantly higher percentage of more severe precancerous lesions, particularly CIN-II and CIN-III. CIN refers to cervical intraepithelial neoplasia, the presence of abnormal cell growth (neoplasia) on the surface of the outer lining of the cervix (intraepithelial tissue). It is also known as cervical dysplasia.
Biologically, having multiple sexual partners can contribute to the abnormality of the vaginal composition of microbes, which impacts the persistent status of HPV. It may also result in the introduction of other sexually transmitted pathogens, such as HIV, which is known to harm our immunity and can also increase the risk of cancer.
Age at First Pregnancy Matters
If people tend to have sex at a younger age and have multiple sexual partners, the risk of getting pregnant at an earlier age increases.
Women with a first pregnancy before 21 years of age were shown in a large-scale study to have a two to threefold increased risk of cervical cancer compared with those who had a first pregnancy after 21 years.
Compared with women who had both their first sex and their first pregnancy after the age of 21, the invasive cervical cancer risk was 2.4 times higher among those reporting their age at first sex and first pregnancy at or below 16 years of age.
Although there was no significant difference across the groups, the data suggested that women with a shorter latency period (age of first sex to first pregnancy of less than two years) may have a slightly higher cervical cancer risk compared with those having a longer gap.
The transformation zone of the cervix is sensitive to hormones, particularly estrogen and progesterone.
During pregnancy, hormonal fluctuations can increase the risk of abnormal changes in the cells of the cervix when HPV is present. This transformation is more likely to happen during a first pregnancy rather than a subsequent one.
Accordingly, both the age at which a woman first engages in sexual activity and the age of her first pregnancy are closely intertwined and together exhibit significantly higher risk estimates for cervical cancer.
Combined Oral Contraceptives Increase Cancer Risk
To avoid an unplanned pregnancy, many women use oral contraceptives. In July 2023, the U.S. Food and Drug Administration approved the first nonprescription oral contraceptive, Opill, a progestin-only pill. Although it does not contain estrogen and is expected to be available over-the-counter in early 2024, it does come with risks and side effects.
Combined oral contraceptives (containing both estrogen and progestogen) are carcinogenic to humans; this assessment was made partly on the basis of the increased risk for cancer of the cervix.
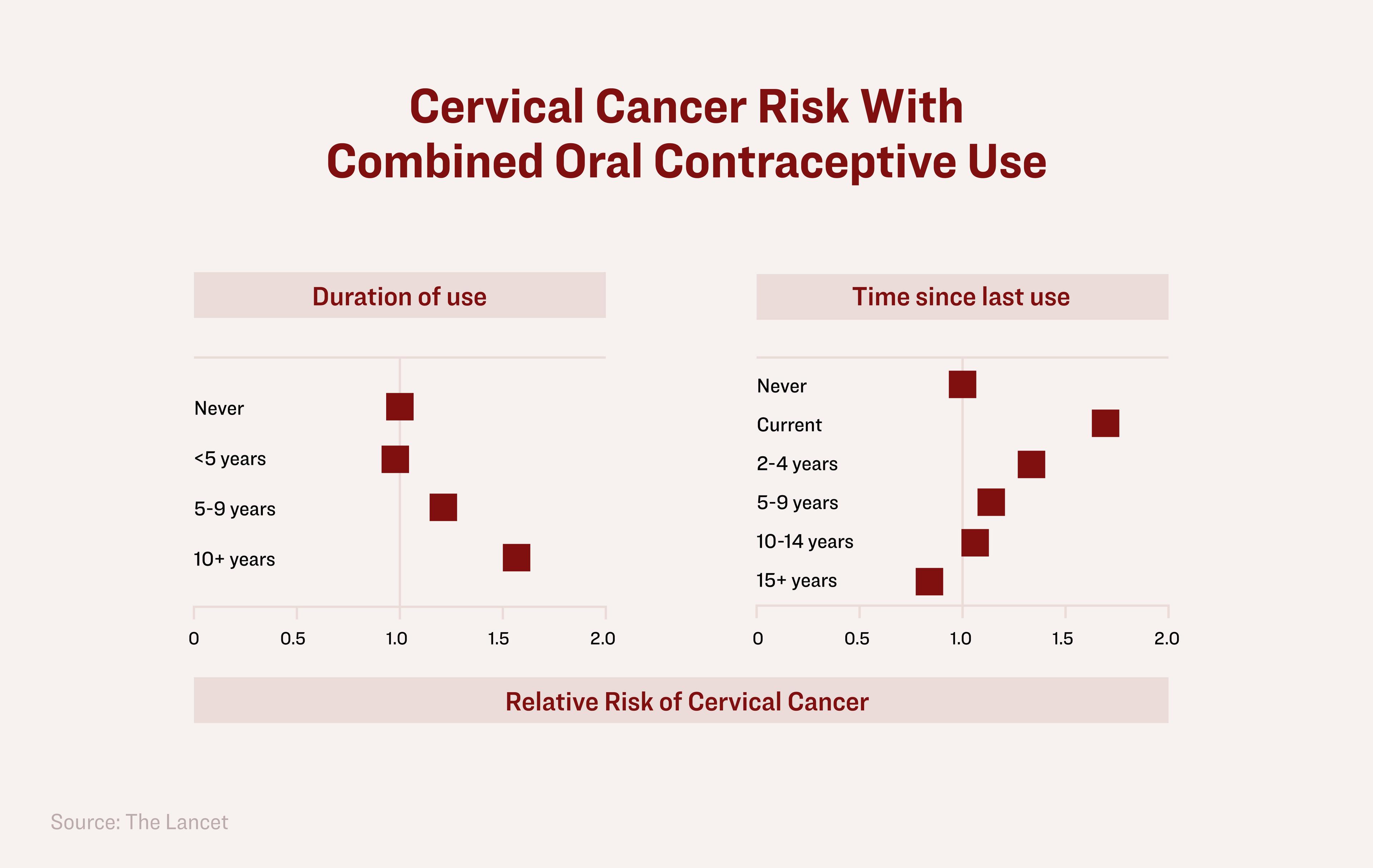
A systematic collaborative reanalysis based on published data from 24 epidemiological studies involving 16,573 women with cervical cancer and 35,509 women without cervical cancer was conducted by IARC to investigate the association between cervical carcinoma and oral contraceptive use. The review was published in The Lancet in 2007.
Researchers found that the relative risk of cervical cancer significantly increased in current users of oral contraceptives and with a longer duration of use, then declined once use subsided.
The relative risk of cervical cancer significantly increases with longer use of combined oral contraceptives. Illustration by The Epoch Times
For example, 10 years of using oral contraceptives started at around age 20 to 30 years is estimated to increase the cumulative incidence of invasive cervical cancer occurring by age 50 by 13 percent in less developed countries and 18 percent in more developed countries.
Cervical cancer also shares several common risk factors with other cancers, including family cancer history, smoking, and a weakened immune system.
Gardasil 9 Doesn’t Protect Against All High-Risk Strains
While the HPV vaccine is a potential way to prevent HPV infection, it could come with serious unexpected consequences.
HPV is a group consisting of over 200 strains. The group is smart and will find a way to survive.
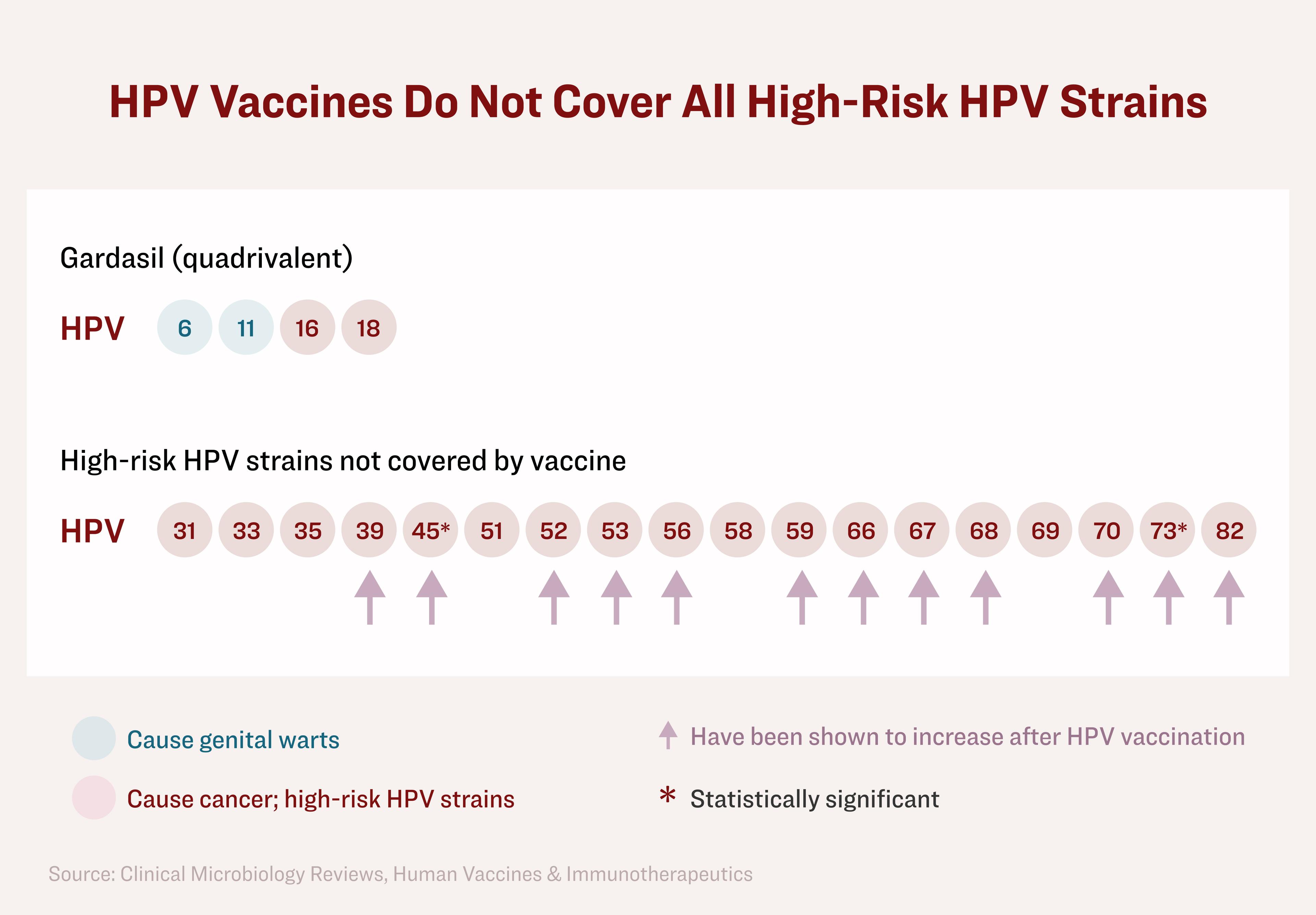
According to a 2015 study conducted by the University of Texas, 22 strains of HPV are associated with a high risk of cervical cancer (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 67, 68, 69, 70, 73, 82, and IS39), but the HPV quadrivalent vaccine covers only two of them; and Gardasil 9 only covers seven strains.
The Gardasil 9 vaccine contains nine HPV strains (6, 11, 16, 18, 31, 33, 45, 52, and 58). Of these, HPV 6 and 11 cause 90 percent of all genital warts, which are not causing cervical cancer; seven HPV strains (16, 18, 31, 33, 45, 52, and 58) are considered high-risk HPV strains. However, there are also “nonvaccine” strains that pose a high risk for cervical cancer, including, but not limited to, HPV 35, 39, 51, 56, 59, 66, and 68.
When people receive the HPV vaccine, the viral strains not covered by the vaccine may become more prevalent and assume a more dominant role in the cervix of the vaccinated women. This means the HPV vaccine has the potential to trigger changes in vaginal microbiota. The virus has found ways to escape vaccine-induced immunity.
The same 2015 University of Texas study found that young adult women who received the HPV quadrivalent vaccine exhibited a higher prevalence of a few nonvaccine but high-risk HPV strains than unvaccinated women, including HPV 39, 45, 52, 53, 56, 59, 66, 67, 68, 70, 73, 82. Among them, HPV 45 and 73 showed a statistically significant increase with a strict analysis.
HPV vaccines do not cover all HPV strains that are associated with cervical cancer and induce changes in cervical HPV strains. Illustration by The Epoch Times
Consequently, the former group remains at risk for other HPV-related cancers associated with nonvaccine strains.
In 2021, more than 10 years after the HPV vaccination program was initiated in most advanced countries, a study in Spain found that HPV 6 and 11 had decreased significantly, HPV 16 also decreased, whereas high-risk strains of HPV 31, 45, and 52 increased significantly. An escalating trend was observed in the nonvaccine strain HPV 51.
Furthermore, a 2021 study published in the Scientific Reports journal by Nature Portfolio found that seven non-HPV vaccine strains (35, 39, 51, 53, 56, 59, 68) were detected in about one-third of black women with cervical cancer, showing most with poor prognosis and lower survival rates.
Uncertain Protection With HPV Vaccines
Despite claims of efficacy, the exact level of protection of HPV vaccines is uncertain.
While the CDC states that “More than 98% of recipients develop an antibody response to HPV types included in the respective vaccines 1 month after completing a full vaccination series,” please do not be misled by this number. These detected antibodies do not protect the cervix directly from an HPV infection. The rate of 98 percent cannot be translated directly into clinical protection.
Our immune system consists of two parts: natural immunity and adaptive immunity. Natural immunity fights a wide range of pathogens like bacteria and other germs regardless of their gene codes, strains, or variants.
HPV vaccines injected into a person’s muscle mainly boost adaptive immunity—more specifically, they stimulate T and B cells and antibodies (also called immunoglobulins) generated by the B cells. There are different types of immunoglobulins, depending on the place where they stay and exert their effects.
In the case of HPV, our innate or natural immunity, especially mucosal immunity, plays a major role in preventing cervical cancer.
(Left) A box of syringes filled with the HPV vaccine. (Fadhli Adnan/Shutterstock) (Right) A box of syringes of the Gardasil vaccine. Ottfried Schreiter/imageBROKER/Shutterstock
Immunoglobulin G (IgG) generated by the HPV vaccine is circulated in the blood. However, the HPV vaccine-induced IgG cannot reach the mucosal area of the cervix to effectively bind with the HPV because it mainly stays in mucosal areas and cervical cancers typically occur at the cervical transformation zone.
The secretory antibody immunoglobulin A (IgA) can play a vital role in mucosal areas to help clear the virus. Even though some studies indicate the existence of IgA or IgG in the cervix, it remains uncertain how local immunity at the cervix protects against HPV infection and cervical cancer in the long term.
Many people argue that the HPV vaccine offers good protection against cervical cancer and is based on solid data. However, their data is not bulletproof and is questionable.
First of all, due to the long lead time from HPV infection to the development of cervical cancer (typically 20 years), conducting a randomized controlled long-term HPV vaccine study is a major challenge. The claims being made for the HPV vaccines are typically based on observational or registry studies.
Observational studies and registry data have shown evidence supporting the protective effects of the HPV vaccine against cervical cancer and precancerous lesions. However, it’s important when interpreting these study results to consider whether data related to the major risk factors previously discussed were collected, analyzed, and balanced across the different study groups.
For example, a study published in the New England Journal of Medicine (NEJM) analyzed data from a Swedish registry to determine the protective efficacy of the quadrivalent Gardasil vaccine for nearly 1.7 million girls and women aged 10 to 30 years. The participants were followed for 11 years.
The study did not adequately assess the major risk factors between the vaccinated and unvaccinated groups (e.g., age at first sex or pregnancy, number of sexual partners, oral contraceptive use, smoking, or general health status).
The NEJM study suggested that the overall level of protection conferred by the HPV vaccine is estimated to be around 60 percent (and up to 88 percent for younger girls). However, as we have previously elucidated, had the main factors associated with cervical cancer risk been included and thoroughly analyzed, the study conclusions would likely have been invalidated.
While some studies may have attempted to account for factors such as age at first sexual activity or age at first pregnancy, monitoring and controlling the number of sexual partners during a long-term HPV vaccine study can be challenging. It would require close monitoring of study subjects and their sexual behaviors over an extended period of time. It is also worth noting that, as of today, studies that have successfully implemented such monitoring and control of sexual activities in their study design are lacking.
Natural Immunity Remains Essential
You may wonder what could happen if you don’t get the HPV vaccine. Will you be left with no protection? Or how will you advise your children to protect themselves against cervical cancer if they do not take the HPV vaccination?
Regardless of whether or not someone receives an HPV vaccination, our natural immunity remains essential to our protection against persistent HPV.
More specifically, our natural immunity against the virus primarily resides with our mucosal immunity.
During the 1918 Spanish flu pandemic, two groups of doctors in Boston and San Francisco conducted separate human challenge trials involving healthy volunteers. Despite employing various aggressive methods, such as dropping mucus or bodily fluids from flu patients into the eyes, noses, or throats of the volunteers, none of the participants became infected with the flu virus.
Amidst the COVID-19 pandemic, a human challenge study involving healthy volunteers was conducted. The study participants were intranasally inoculated with the SARS-CoV-2 virus. Surprisingly, only 53 percent of them became infected with mild symptoms, while the other half remained uninfected.
(Left) Spanish Flu 1918: Nurses care for patients who are being treated with an outdoor fresh air cure during the Spanish Flu in Lawrence, Mass., in 1918. (Hulton Archive/Getty Images) (Right) A microscopic view of the COVID-19 coronavirus at the Centers for Disease Control and Prevention in Atlanta. CDC/Getty Images
Natural immunity does not only fight against the virus, it also fights against cancer.
Our bodies are naturally equipped with a defense system that can fight cancer cells. The key lies in optimizing our natural immunity, thus enabling a strong immune system that can promptly detect and monitor any signs of cancer cells.
There is significant evidence suggesting the indispensable role of our natural immunity in cancer surveillance.
Active clinical programs targeting innate immunity in cancer therapy as of September 2019 include four modes of action: drugs that capitalize on antimicrobial immunity for tumor control; drugs that induce or amplify the innate immune response; drugs that promote the effector responses of innate immunity; and drugs that relieve immune suppression at the tumor bed.
Tumor detection induces activation of innate immune cells which promote antibody effector functions and tumor cell destruction. In addition to their direct tumoricidal effect, tumor-activated innate immune cells participate in all steps of T-cell generation and activity against cancer cells by participating in tumor-specific T-cell priming, expansion, and infiltration at the tumor site.
In our battle against cancer, it is crucial to maintain a constant focus on strengthening our immune system and exerting control over known risk factors. Adopting a holistic approach is actually the most important thing we can do—with zero side effects. Eating healthy food, maintaining quality sleep and a healthy weight, exercising, mindfulness programs, meditation, and stress-reduction techniques are all helpful to our immunity.
The strategy of only targeting the virus is not as smart as focusing on enhancing our natural immunity, as our immunity is dynamic, resourceful, and able to combat numerous viral variations, especially when the virus keeps changing after HPV vaccination.
Our Choices Matter
There are undeniable safety risks associated with HPV vaccines. One of the most difficult questions is deciding whether these risks outweigh the benefits.
As we discussed in Part 3, the so-called risk-benefit analysis of the HPV vaccine is not valid when the control group is given a placebo containing a toxin, such as aluminum, which was proven to cause injuries.
The HPV vaccine is not a golden shield protecting against cervical cancer. Its claims of protection are highly questionable and its harms are well-documented.
Furthermore, a Pap smear test used for screening has contributed to a decline in cervical cancer death rates, even before the introduction of the HPV vaccination. Cervical screening is an established secondary prevention tool that leads to the removal of precancerous lesions before they become cancerous.
Let’s instead wisely focus our attention on how to strengthen our immunity and avoid the high-risk behaviors with the greatest impact on our cervical health. Maintaining responsible attitudes towards sexuality is an effective and natural way to protect ourselves.
We all possess a sacred gift—our naturally endowed immunity. By controlling our risk behaviors and bolstering our natural immunity, we can confidently embrace a more holistic, dynamic, and robust approach to safeguarding ourselves against HPV infection and cervical cancer.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.