Symptoms of Dry Eye Disease
In order to function properly, eyes need to keep their ocular surface moist. When the eyes lose the ability to maintain an adequate film of moisture at this surface, pain, irritation, and other symptoms occur. The biochemical processes involved in maintaining healthy ocular surfaces are intricate. Like any body system, disruption of the delicate balance of these processes can lead to disease.The severity of eye irritation for DED sufferers ranges from mild irritation to severe pain. There may be a scratchy feeling, or a foreign body sensation, where it feels as though there is something in the eye. The eyes may feel gritty and may sting or burn. The blood vessels may be pronounced, making the white part of the eyes red.
Dry eyes are frequently sensitive to light, and for some individuals, bright light may feel unbearable. Dry eyes may feel tired and heavy. Blurry vision is another potential symptom of the disease.
When the eye is irritated because of DED, an inflammatory cascade is set in motion: Inflammatory chemical messengers, called cytokines, are released, and helper T cells are recruited to the ocular surface. This causes discomfort and adds an additional strain on the body.
Risk Factors for Dry Eye Disease
Anyone can get DED, but your risk of getting the disease increases with certain factors.Nonmodifiable risk factors include being over 50 years old, being female, being of Asian ethnicity, having meibomian gland dysfunction, having connective tissue diseases, and having certain autoimmune conditions such as Sjogren’s syndrome.
In addition, a diet low in omega-3 fatty acids and refractive surgery are likely to contribute to increased risk for developing dry eye.
Dry Eye Syndrome Tear Film
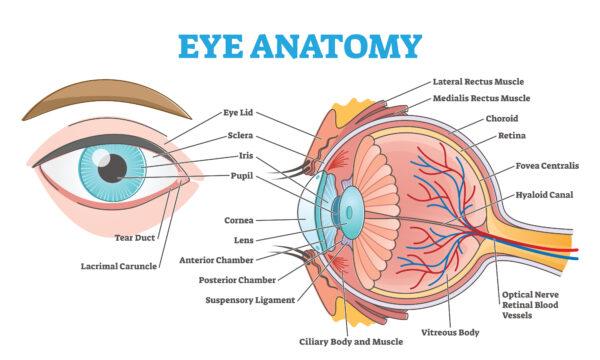
The cornea and sclera make up the outer covering of the eyeball. The cornea is a transparent dome covering the front surface of the eye. Light must travel through the cornea to enter the eye, where it will be focused on the back of the eye in a region called the retina.The sclera is the white outer layer of the eye. It’s continuous with the cornea. This area is protected by a somewhat three-layered structure of fluid known as the tear film.
The tear film provides lubrication and hydration for the cornea and sclera. It also provides oxygen, antimicrobial enzymes called lysozymes, and antibodies. The antibodies fight against bacteria, viruses, and parasites.
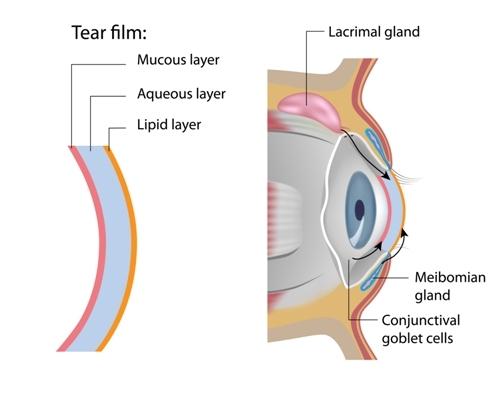
Normal tear film has three layers: an outermost lipid layer, a watery middle layer, and a mucous inner layer.
The outermost lipid layer of the tear film is made of oily secretions from the meibomian glands, which are little oil glands located along the margins of the eyelids. The margins are the edges that touch when you close your eyes.
As oil is less dense than water, it floats to the surface of the tear film and provides a key barrier to the evaporation of water from the tear film.
The aqueous, or watery, middle layer of the tear film is just under the oily layer. It’s produced by secretions from the lacrimal gland, located superior and lateral to each eye. In addition, there are many accessory lacrimal glands in the conjunctiva—the clear tissue overlaying the white part of the eye—which contribute water to the aqueous portion of the tear film.
The innermost mucin layer is made predominantly by goblet cells in the conjunctiva. This mucous portion of the tear film interacts with the surface of the cornea to allow the tear film to spread uniformly across the cornea with each eye blink.
Aqueous Deficiency in Dry Eye Disease
Aqueous deficiency is a type of DED resulting from a decreased production of the watery portion of the tear film from the lacrimal glands. It represents only 10 to 15 percent of DED cases.Meibomian Gland Dysfunction and Dry Eye Disease
Most cases of DED are due to meibomian gland dysfunction (MGD) and problems with the oily lipid layer of tear film they produce. Meibomian glands are the sebaceous (fat secreting) glands located along the margin of the eyelids. They secrete meibum, which is made of phospholipids, cholesterol, wax esters, and other lipids, forming the oily outermost layer of the tear film.If the proper lipid components in the tear film aren’t present, the tear film may evaporate too quickly and cause DED.
While that sounds straightforward, the underlying etiology of MGD is a tremendously complex pathology with interplay between multiple biological pathways at the ocular surface.
These researchers describe how they think the cycle begins: Microbiological changes cause meibomian gland blockage. If untreated, the glands may atrophy and become unable to produce adequate, if any, meibum. The resulting tear film becomes unstable, as it lacks the proper components of the lipid layer, and DED ensues.
The inflammation associated with MGD and DED exacerbate both situations, leading to more biochemical pathway dysfunction. In a sense, it’s a cascade of dysfunction that continues to get worse and worse if left untreated.
Aqueous deficiency can trigger MGD; thus in some individuals, both conditions exist together.
Lid margin inflammation, called blepharitis, is a cause of, and an effect of, MGD. Seborrheic dermatitis, rosacea, staphylococcal infections, and Demodex folliculorum mites may be causative factors of the blepharitis, or secondary (and exacerbating) factors due to blepharitis being present and the health of the eyelid margin being compromised.
Other factors can affect meibomian gland function. For instance, androgens, generally, stimulate the secretion of meibum. Individuals in androgen-depleted states have altered meibomian gland secretion. Furthermore, it’s been known for 30 years that 13-cis-retinoid acid (Accutane), is linked with severe meibomian gland atrophy (Mathers et al., 1991).
Where to Go From Here Dry Eye Disease
Aside from the (sometimes severe) irritation and pain of DED, there’s the risk of corneal damage. All light coming into the eyeball needs to pass through the cornea for vision to ensue. The cornea is an extremely delicate tissue that can become greatly damaged by MGD and DED.When the cornea begins to scar, from ongoing inflammation and mechanical damage, such as may occur when the tear film is unstable, it loses its transparency and smooth surface, resulting in cloudy and distorted vision.
Your eyes are incredible organs that allow you to view the world around you. It’s vital that you invest in protecting your eyes.
There are numerous treatment options for those with DED, but it can take time to figure out which treatment works best for your specific situation. There are many factors that play into ocular surface disease and more than one biochemical pathway is typically dysregulated.
Dr. Laura M. Periman is a board-certified ophthalmologist, fellowship-trained cornea and refractive surgeon, and ocular surface disease expert. She has treated many patients with DED and emphasizes that dry eye is a multifactorial disease.
She states: “Dry Eye Disease is like a giant circus tent with about 30 different animals inside running amok and the lights are off. The challenge for the clinician is to identify which animals are creating the most mischief and address them as directly as possible.”
Individuals with dry eye symptoms may need to visit a few ophthalmologists to find one who really understands DED. The key is persistence and a willingness to try recommended procedures and treatments until you find the one that works best for your eyes.
Periman’s advice to any person suffering from DED is simple, but important: “Pay consistent attention to the five pillars of wellness: nutrition, hydration, sleep hygiene, exercise, and mindfulness.”
Aggarwal, S., & Galor, A. (2018). What’s new in dry eye disease diagnosis? Current advances and challenges. F1000Research, 7, F1000 Faculty Rev-1952. https://doi.org/10.12688/f1000research.16468.1
Barabino, S. (2022). Is dry eye disease the same in young and old patients? A narrative review of the literature. BMC Ophthalmol 22, 85. https://doi.org/10.1186/s12886-022-02269-2
Baudouin, C., Messmer, E. M., Aragona, P., Geerling, G., Akova, Y. A., Benítez-del-Castillo, J., Boboridis, K. G., Merayo-Lloves, J., Rolando, M., & Labetoulle, M. (2016). Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of meibomian gland dysfunction. The British journal of ophthalmology, 100(3), 300–306. https://doi.org/10.1136/bjophthalmol-2015-307415
Chang AY, Purt B. Biochemistry, Tear Film. [Updated 2022 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572136/#
Chhadva, P., Goldhardt, R., & Galor, A. (2017). Meibomian Gland Disease: The Role of Gland Dysfunction in Dry Eye Disease. Ophthalmology, 124(11S), S20–S26. https://doi.org/10.1016/j.ophtha.2017.05.031
Dana, R., Bradley, J. L., Guerin, A., Pivneva, I., Stillman, I. Ö., Evans, A. M., & Schaumberg, D. A. (2019). Estimated prevalence and incidence of dry eye disease based on coding analysis of a large, all-age United States Health Care System. American Journal of Ophthalmology, 202, 47–54. https://doi.org/10.1016/j.ajo.2019.01.026
Findlay, Q., & Reid, K. (2018). Dry eye disease: when to treat and when to refer. Australian prescriber, 41(5), 160–163. https://doi.org/10.18773/austprescr.2018.048
Mathers, W. D., Shields, W. J., Sachdev, M. S., Petroll, W. M., & Jester, J. V. (1991). Meibomian gland morphology and tear osmolarity: changes with Accutane therapy. Cornea, 10(4), 286–290. https://doi.org/10.1097/00003226-199107000-00002
Um, S. B., Yeom, H., Kim, N. H., Kim, H. C., Lee, H. K., & Suh, I. (2018). Association between dry eye symptoms and suicidal ideation in a Korean adult population. PloS one, 13(6), e0199131. https://doi.org/10.1371/journal.pone.0199131