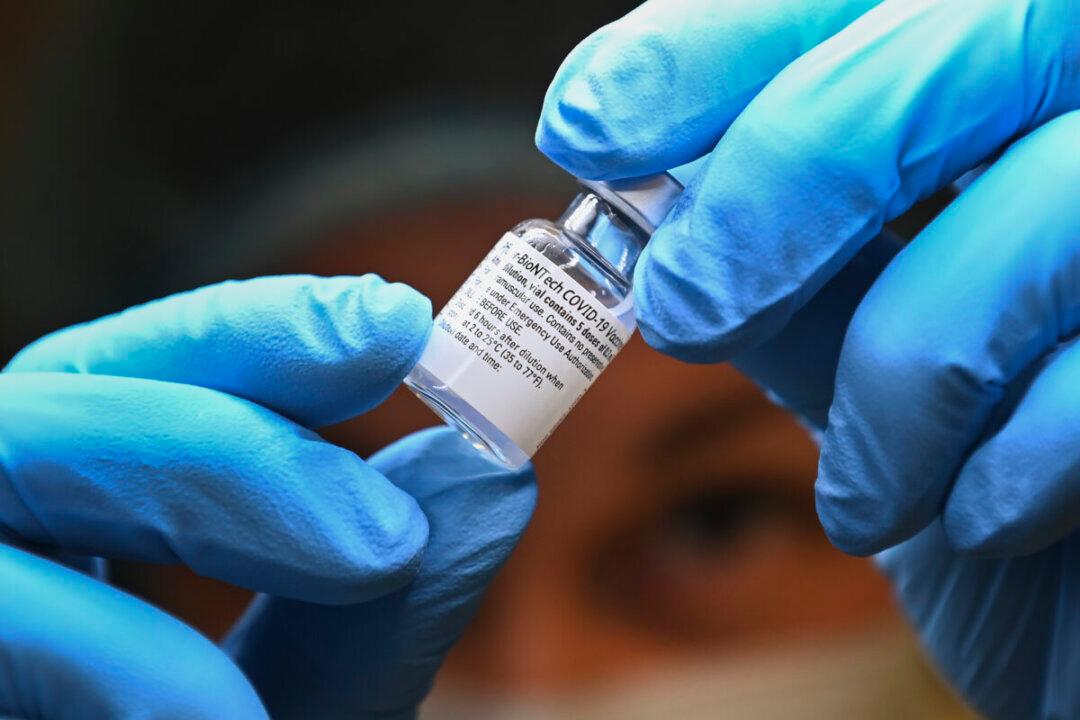
Recently both Pfizer and Moderna announced they were developing a combination injection utilizing mRNA coding for the BA4/BA5 Omicron subvariant and new mRNA coding for antigens contained in the influenza virus.[i]
Because the COVID-19 component is under Emergency Use Authorization, has failed animal data and no human studies, that component should be off the table from the start.