

The Food and Drug Administration (FDA) recently approved the first COVID-19 drug for children under the age of 12–remdesivir, which has always been a controversial drug. Now, with its use in infants and young children, is the controversy over remdesivir already gone?
- Hospitalized
- Children who are not hospitalized, but have mild to moderate symptoms and are at high risk of developing severe illness or death
In particular, children (especially newborns) have limited expression and cannot clearly express physical distress, so it is difficult for parents and pediatricians to determine whether an infant is mildly or moderately ill or at risk of becoming seriously ill.
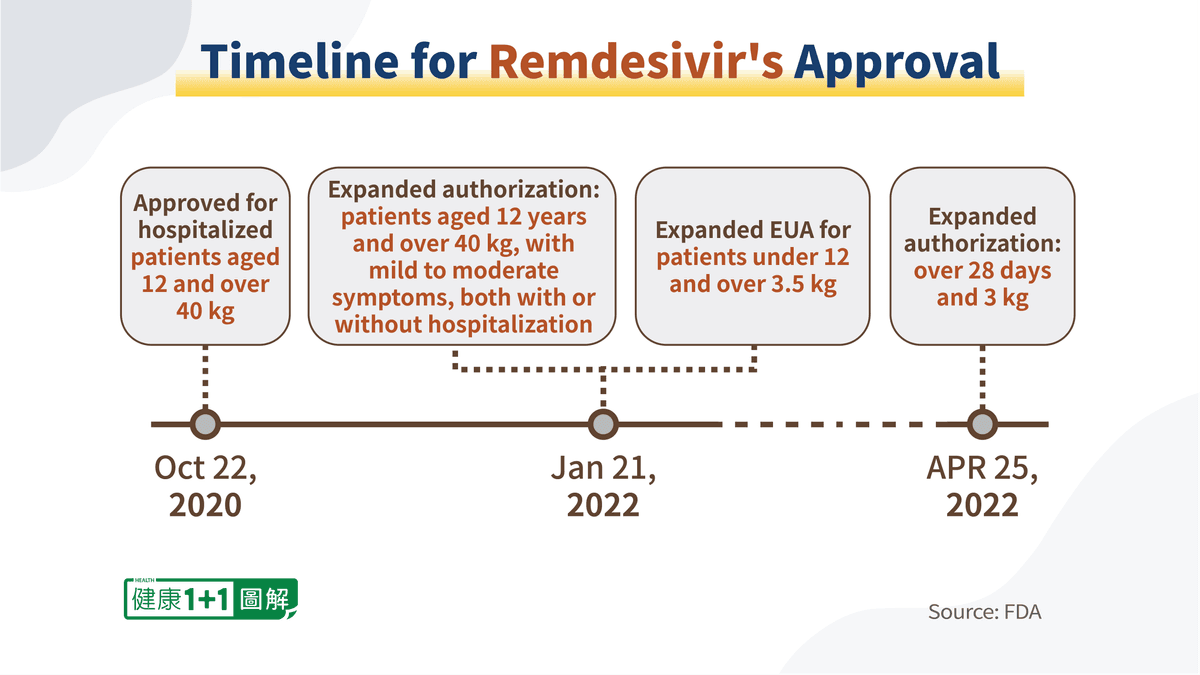
Timeline for Remdesivir’s Approval
In as early as October 22, 2020, remdesivir received emergency approval from the FDA for use in adults and adolescents aged 12 years and over 40 kilograms, who are hospitalized with the COVID-19 infection.By January 21, 2022, remdesivir had received two expanded authorizations.
On April 25, 2022, remdesivir received a full authorization allowing its use in infants, toddlers and adolescents over 28 days and 3 kilograms, both hospitalized and non-hospitalized with mild to moderate symptoms.
Remdesivir’s Pediatric Clinical Trial Data Are Astonishing
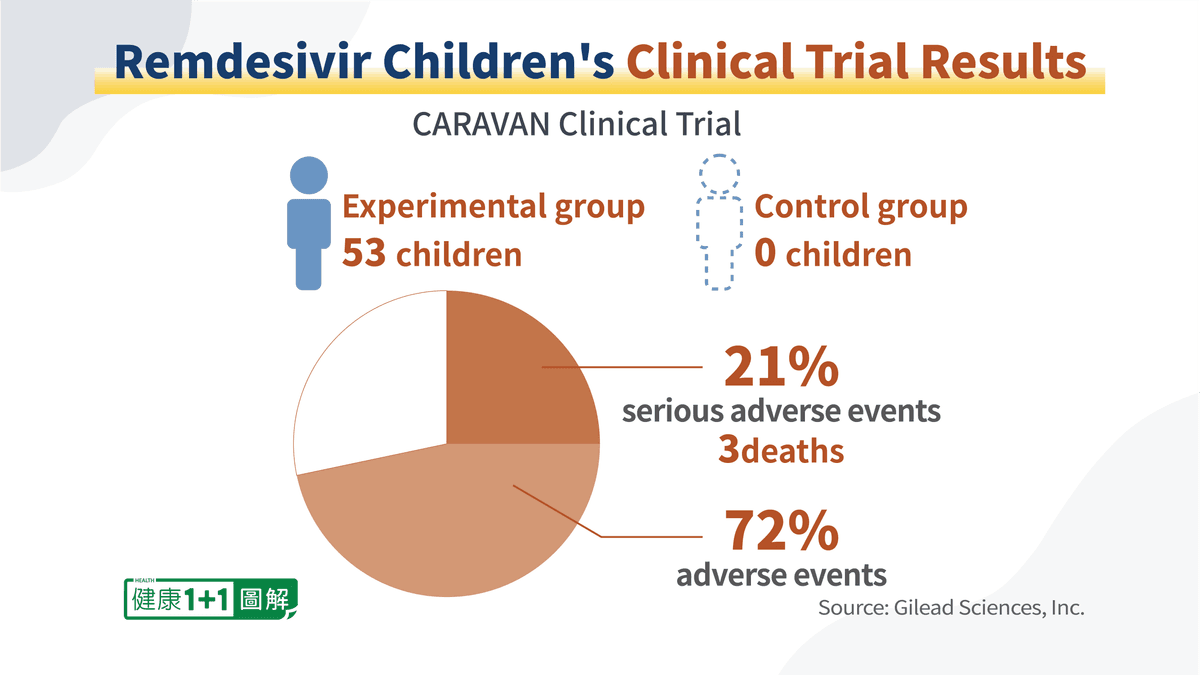
In order to obtain the FDA’s authorization, Gilead Sciences, Inc. published data from a clinical trial called CARAVAN, which was jointly conducted by research centers in different countries.Unlike many trials with double-blind control groups, this clinical trial was very simple in design, as there was no control group. In addition, the total number of children participating in the trial was only 53.
The trial discovered that in this small population, 72 percent of the children experienced various adverse events, such as shortness of breath and rash; and nearly 21 percent experienced serious adverse events, including three deaths. The study emphasized that serious adverse events were not considered to be directly related to the drug, and that deaths were caused by other diseases.
Nevertheless, during the clinical trial, children were not allowed to receive any other drugs at the same time. What caused the serious adverse events in 21 percent of the children, besides remdesivir? If no reasonable explanation is given, and the possibility is simply denied, it is hard not to believe that these serious adverse events were not related to the drug.
In addition, since the number of participants in the trial was very small, it is impossible to separate the participants into groups of recipients of 5 mg/kg and recipients of 1 mg/kg for a controlled trial, in order to analyze whether reducing the dose of the drug would reduce the harm to children. And this should have been a fundamental consideration. The approved dose to weight ratio for remdesivir in infants and children is 5 mg per kilogram of body weight, the same ratio as for adults.
Questionable Trial Conclusions: Is Remdesivir Less Effective Than a Placebo?
Remdesivir has always been said to be effective in the treatment of early-stage patients.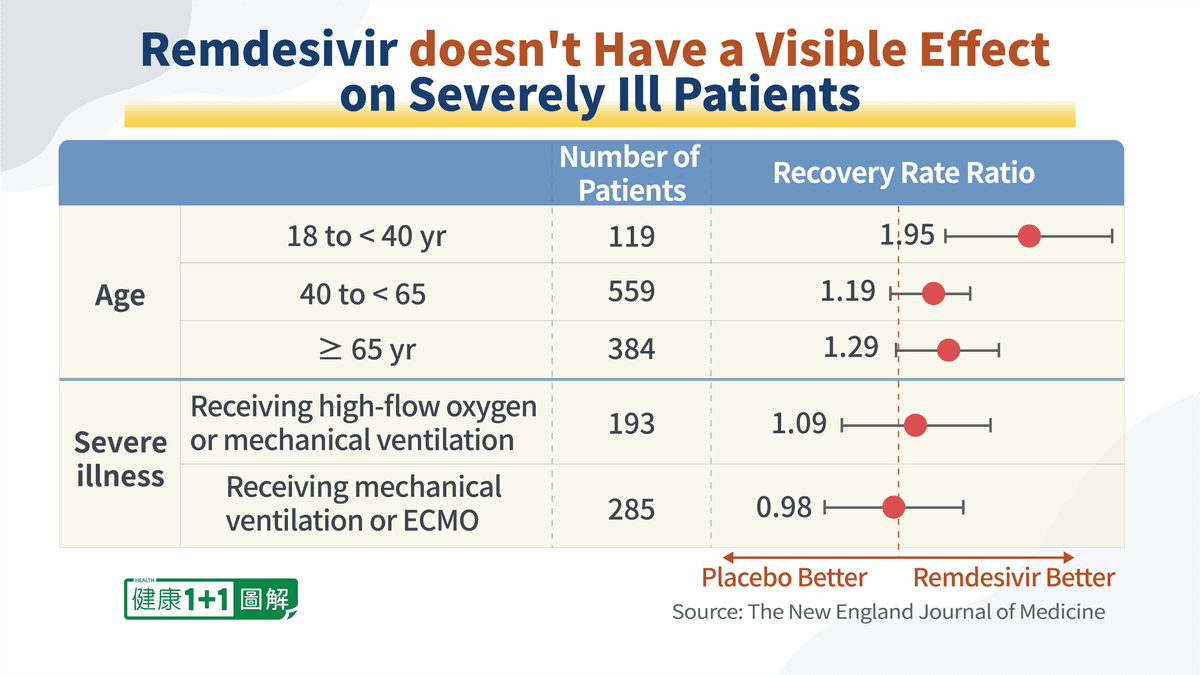
This trial found that the effectiveness of remdesivir in treating severe illness was very limited.
In cases of respiratory distress requiring mechanical ventilation, that is, non-invasive respiratory assistance, the recovery rate of the treatment group, who received remdesivir was only marginally better compared to the control group, who received the placebo, with a ratio of 1.09:1.
In the case of patients who required mechanical ventilation, remdesivir was found to be even slightly less effective than the placebo.
This shows that remdesivir doesn’t have a visible effect on severely ill patients. Therefore, even if remdesivir receives full FDA approval, the main emphasis should still be on the efficacy of the drug in treating early-stage patients.
The PINETREE trial concluded that remdesivir “resulted in an 87% lower risk of hospitalization or death than placebo.” How did this figure come about? This figure was obtained only from the treatment of elderly people over 60 years of age. And the report’s conclusion didn’t emphasize that the drug is more effective in treating people from this age group.
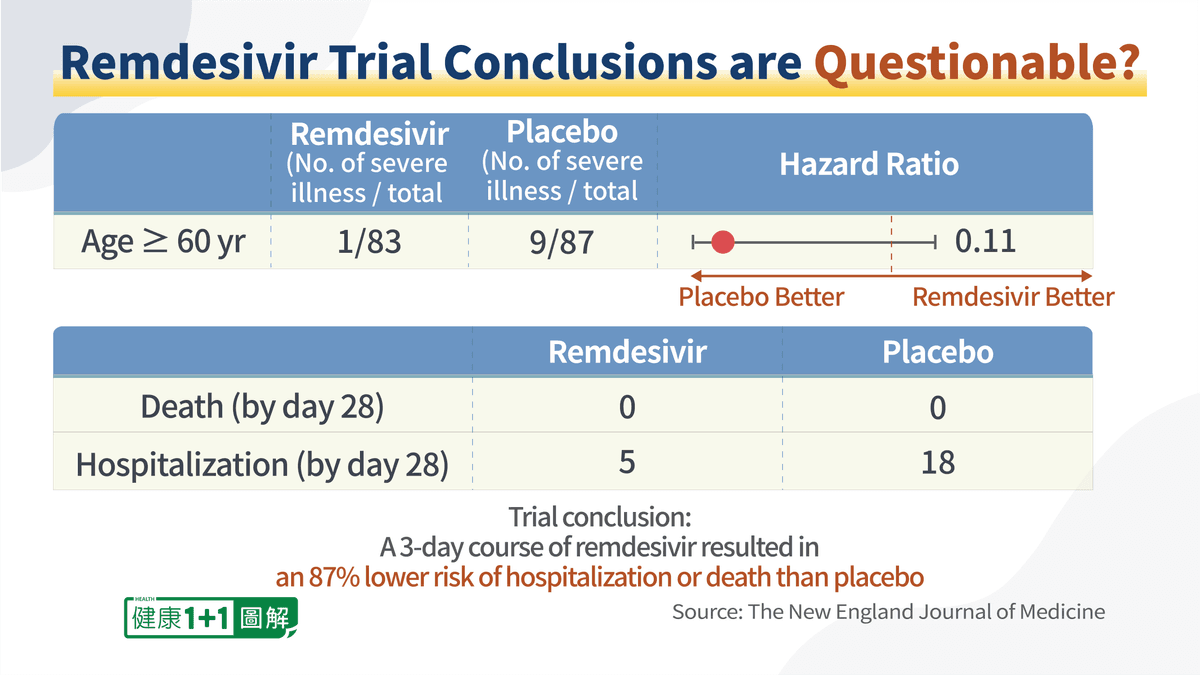
Moreover, no one in the experimental group or the control group died, so how can we conclude that remdesivir can protect patients against death?
Although the report’s conclusion is eye-catching, from a scientific point of view, it is not rigorous and may be misleading to the public.
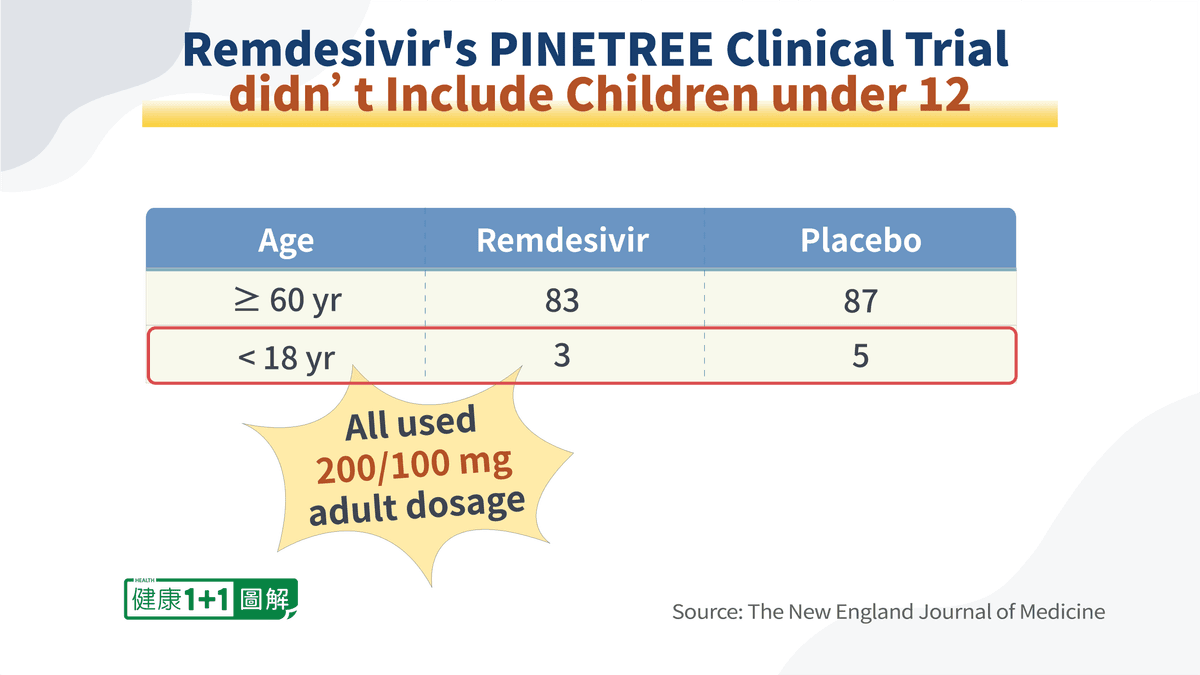
The two aforementioned clinical trials were the primary basis for remdesivir to obtain the FDA approval, and they did not include any data on children under the age of 12.
Remdesivir’s Side Effects Include Severe Kidney Failure
The controversy over remdesivir has been focused on the issue of side effects.- Allergic reactions:
- Changes in heart rate
- Rash, fever, nausea, and shortness of breath
- Swelling of the lips, face, and throat, as well as shivering
- Increased liver enzymes, which is a sign of liver function impairment
This large percentage of risk of serious side effects is very difficult for the medical community to accept, which is why many countries question the widespread promotion and use of remdesivir.
In addition to the side effects of hepatic (liver) function impairment, there have been many reports of acute renal failure and kidney injury associated with remdesivir.
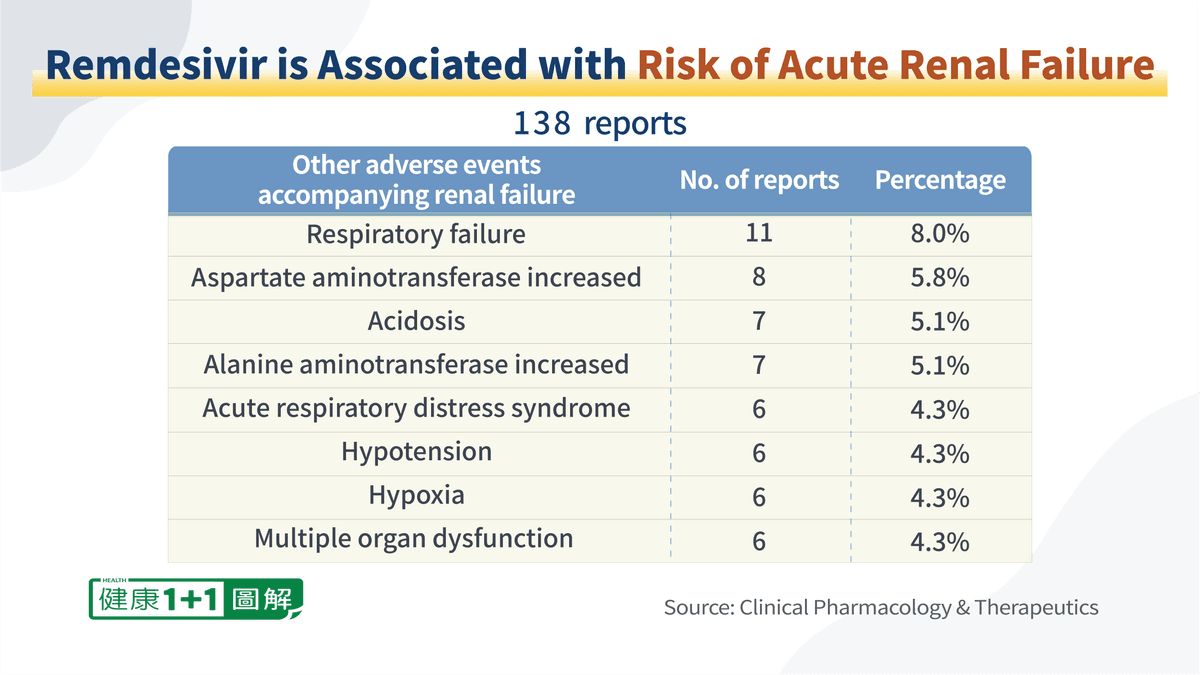
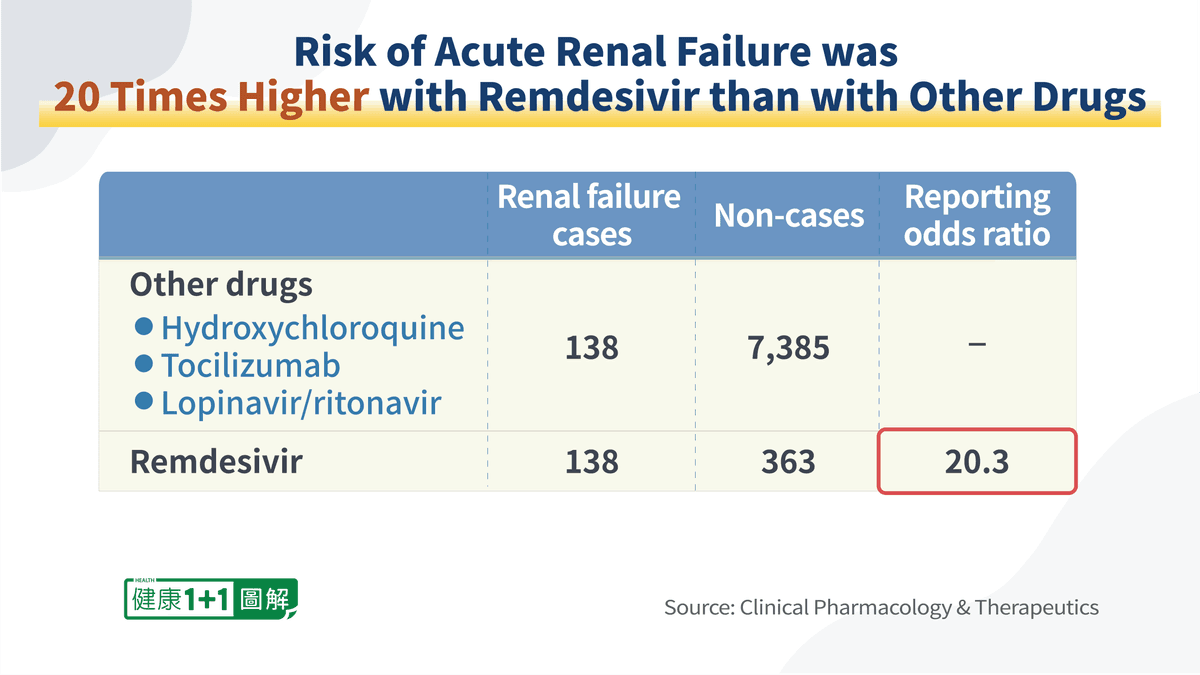
A comparison of remdesivir with other commonly used COVID-19 drugs, including antivirals, monoclonal antibodies, and hydroxychloroquine, showed that the risk of renal failure was 20 times higher with remdesivir than with other drugs.
Among the adverse events related to renal injury, there are other more serious long-term conditions besides acute renal failure, such as renal injury and chronic renal failure. Although the probability of developing these conditions is not very high, these are serious conditions.
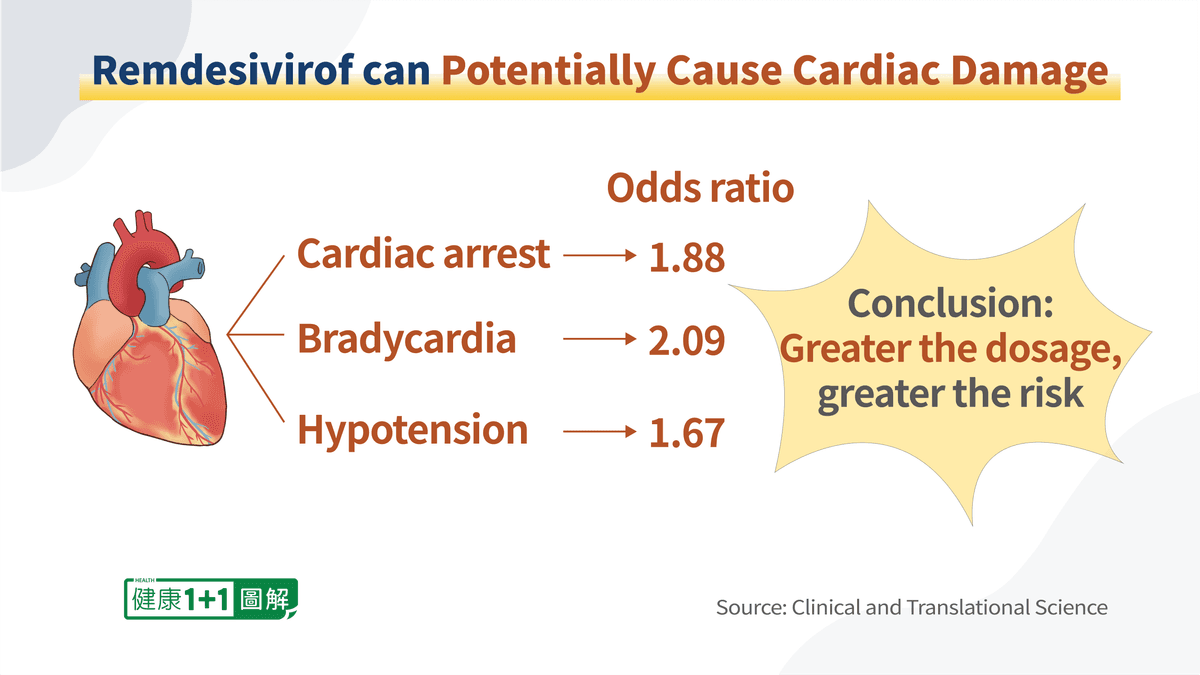
This suggests that the dosage is very important and that simply administering the drug to children in the same dose-to-weight ratio as adults may put the children’s hearts at great risk.
Furthermore, the public is concerned about the toxicological analysis and studies of remdesivir in fetuses, newborns, infants, as well as in breast milk. Gilead Sciences, Inc. also mentioned in the Patient Information that it was not certain whether or not remdesivir would harm fetuses or whether or not the drug would enter breast milk. In general, before a drug can be tested in vivo, animal testing must be completed, to see if the drug causes any harm to the animals’ development. However, remdesivir has not undergone such tests.
The current controversy over the side effects of remdesivir seems to be ignored, and the FDA has authorized the use of this drug in infants and young children over 28 days of age, which I believe poses a significant risk.



