The skin is a formidable barrier with attributes far beyond the potential workings of scientists or chemists. It is strong but supple, it fixes itself when damaged, and it changes color to adjust to the climate.
The skin is more active than many people realize; it even synthesizes various compounds, including immunoglobulin A, an antibody important in immune defense systems.
It isn’t just a covering, but plays diverse roles in the body—from helping to regulate body temperature to initiating the process of vitamin D production. The skin’s absorptive property allows it to take in things from the environment, such as beneficial medicines or harmful toxins.
Our skin is an impossible harmony of specialized cells working in an intricate synergy. There are likely other functions of the skin we haven’t even begun to understand. It’s one of our most visible organs, yet few people know much about what skin looks like below the surface or how it functions.
A Quick Overview
The skin is part of the integumentary system, which also includes hair, nails, and certain exocrine glands, such as the sweat glands. It forms a physical barrier between the environment outside our body and our internal body structures, such as muscles, bones, and other organs.The skin has to have strength and durability but must also be flexible and able to repair itself. Three layers work together to accomplish these goals: the epidermis, the dermis, and the hypodermis. Let’s take a closer look at each layer and its specialized functions.
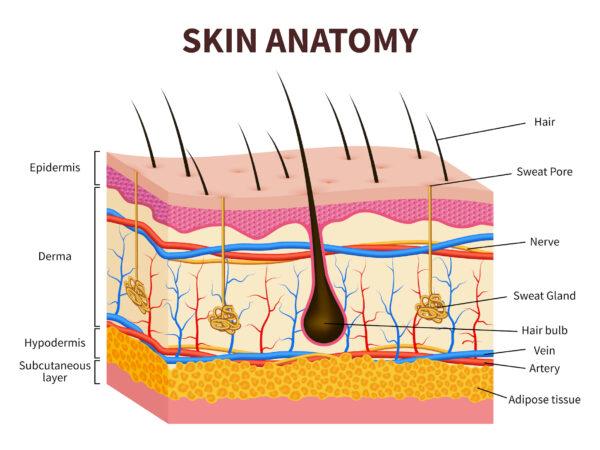
Epidermis
The epidermis is the outermost layer of skin. This is the layer you see when you look at yourself, and it’s formed predominantly by special cells called keratinocytes.Just as the name implies, these cells produce a substance called keratin, a protein that’s durable and doesn’t dissolve in water. You’re familiar with this protein because your hair is made of keratin. Keratinocyte stem cells, located in the lower epidermis, divide and form keratinocytes. The keratinocytes get pushed up toward the surface of the skin as new keratinocytes form beneath them. As the keratinocytes mature, they produce lots of keratin and become packed with this protein.
Keratinocytes assemble together tightly. The closer they get to the skin’s surface, the tighter they’re crammed, forming a seal that creates a waterproof barrier. It takes about four weeks for keratinocytes to move to the surface of the skin from the time they were created deep in the epidermis. This means you have a new covering of epidermal cells every month.
Due to the process of ongoing keratinocyte production, we continually replace the cells that flake off when the skin is rubbed. It’s an interesting process that has to be tightly regulated, as the consequence of unregulated keratinocyte creation would be skin that’s too thin or too thick.
Increased rubbing triggers epidermal cells to grow faster. If the rubbing doesn’t increase the amount of skin flakes that are shed, the cells can build up, resulting in a callus—an area of thickened skin. This is a protective mechanism that allows our bodies to adapt to environmental stimuli to protect us.
Calluses are a form of hyperkeratosis—a condition where the outer layer of skin thickens. Hyperkeratosis not only results from normal use, like calluses do, but can also occur in the pathology of eczema, psoriasis, certain autoimmune disorders, and arsenic poisoning.
Keratinocytes synthesize vitamin D when exposed to ultraviolet (UV) radiation. Vitamin D3 is formed when UV radiation converts 7-dehydrocholesterol into vitamin D3 in keratinocytes. Vitamin D3 made in the epidermis gets transported to the liver, where it gets metabolized into the most common circulating form of vitamin D in your body, called 25-hydroxyvitamin D (calcidiol). Your kidneys convert 25-hydroxyvitamin D into a more potent metabolite called 1,25-dihydroxyvitamin D (calcitriol) for use in numerous body functions. One such function of vitamin D is to increase calcium absorption from the gut, making this vitamin critical for proper bone formation.
The epidermis is made up mostly of keratinocytes, but it also contains several other cell types.
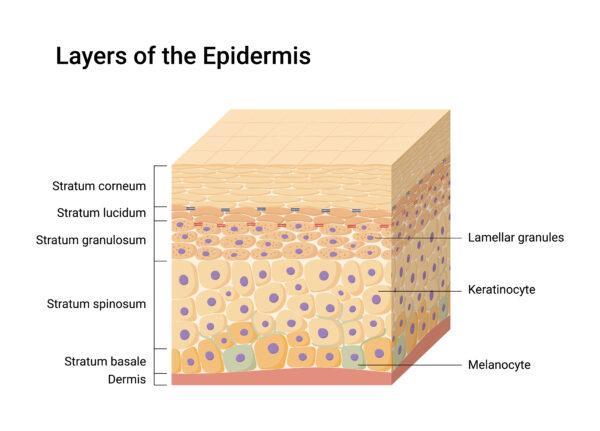
One of these other cell types is melanocytes, which produce a black pigment called melanin. Increased exposure to sunlight results in melanocytes producing more melanin, causing the skin to become darker.
This is another example of how our skin responds to environmental stimuli to protect us—in this case, from UV radiation from the sun. The continuum of light brown to dark brown skin color present in our population is due to genetic influences on melanin production and storage.
Many people assume that individuals with darker skin tones must have more melanocytes; however, if you compare a body region in a dark-skinned person versus a light-skinned person—take the forearm, for instance—the relative concentration of melanocytes in their tissue is remarkably similar. What’s different, however, is the number of pigment-containing organelles, called melanosomes.
In individuals with African ancestry, melanosomes are generally larger in size, more pigmented, and more numerous in the epidermal tissue, as compared to individuals with European ancestry. The melanosomes are created by the melanocytes and then transferred to keratinocytes, giving the skin a specific shade of brown.
Vitiligo is a condition in which melanocytes in an area of skin either die or just stop producing melanin. The skin in this area then looks lighter than the skin around it. This can affect people of all skin types. It’s not contagious or life-threatening.
In addition to keratinocytes and melanocytes, the epidermis contains Langerhans cells, which are involved in immune function.
Langerhans cells have a unique shape. They have long, dendritic projections, like arms, that reach way out between keratinocytes and extend toward the surface of the epidermis. You can imagine them as little octopuses that use their long arms to sense what’s going on in the tissue around them. The network formed by these cells is dense.
Microbes trying to get into the body through the skin will inevitably encounter these Langerhans cells. When the Langerhans cells sense microbial activity, they quickly initiate antimicrobial responses. Keratinocytes can alert Langerhans cells to danger by releasing little chemical messengers called cytokines. Other immune cells, called T-lymphocytes, also reside in the epidermis and can activate the immune system to protect the body from microbes.
The community of cells in the epidermis is like a close-knit neighborhood. The cells communicate in an ongoing manner to ensure the neighborhood is safe from invaders.
As with any neighborhood, things can go wrong in the epidermis when communication goes awry. Psoriasis is one such example.
Psoriasis is an autoimmune disorder of the skin. While the etiology, or cause, of psoriasis is not entirely clear, what we do know is that T-lymphocytes in the epidermis are triggered to become overactive and start signaling uncontrollably. When the T-lymphocytes start releasing excessive amounts of cytokines, this initiates an inflammatory process in the skin.
In healthy skin, localized inflammation is an important part of the immune response to a microbial threat or damage to the skin, such as a cut.
In an individual with psoriasis, however, this inflammatory response occurs when there is no microbial threat or skin damage. It sets off a cascade of molecular reactions, resulting in dilated blood vessels and an inpouring of immune cells. Keratinocytes respond strongly to the cytokines and begin releasing their own cytokines. The result is further immune amplification, which damages the tissue. Keratinocytes receive messages to multiply rapidly.
Dermis
Just beneath the epidermis is the dermis, the middle layer of skin. The dermis has blood vessels along with lymph vessels, sweat glands, nerves, and hair follicles. It has many functions, but of particular importance is the role it plays in regulating body temperature.Blood vessels in the dermis dilate, or enlarge, when the body starts heating up due to exercise or hot temperatures. This allows a greater volume of blood to circulate near the skin’s surface, effectively releasing heat. Cooler temperatures cause the blood vessels to constrict, helping keep heat from being lost.
In addition, the dermis helps to cool the body through releasing sweat. The evaporation of water molecules in sweat pulls heat from the skin, and your body capitalizes on that process to cool you down.
The dermis is divided into the superficial papillary region and the deep reticular region. The superficial (meaning closer to the skin surface) papillary dermis is on top, closer to the epidermis. The papillary dermis has finger-like projections that reach into the epidermis. Collectively they’re called dermal papillae, which help create a tight adherence between the epidermis and dermis, and keep the epidermis from being able to slide horizontally across the dermis.
If the skin is rubbed extensively, like when you use a rake for several hours, these finger-like projections pull away from the epidermis. Extracellular fluid builds up in the gap, forming a blister.
The superficial papillary dermis has some fat cells, called adipocytes, and an abundance of capillary loops—horseshoe-shaped blood vessels that supply the tissue with oxygen-rich blood.
This layer also has phagocytes to help protect the skin against microbes.
Underneath the superficial papillary dermis is the deep reticular layer of the dermis. This layer is tough and is made up of a dense network of elastin and collagen fibers.
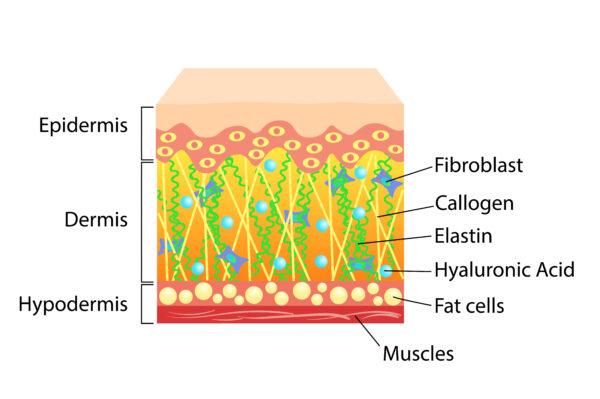
The elastin fibers give skin its elasticity, so there’s some movement and flexibility in skin. If skin is stretched too much—for example, on the abdominal skin of a pregnant woman—the dermis can tear. The result is stretch marks.
The collagen fibers give skin its tensile strength and firm structure. Each collagen fiber is formed by three long protein fibers supercoiling into a triple-helix conformation. The collagen fibers in the deep reticular layer extend up into the superficial papillary dermis and down into the hypodermis, making these layers strong and tightly adhered. Collagen also binds water, keeping skin hydrated.
Excessive exposure to UV rays from the sun can damage collagen fibers and cause them to break down more quickly than normal. The chemical bonds, called peptide bonds, within the collagen protein actually get broken, creating a much more unstable collagen fiber. The skin then doesn’t have the same durability and loses its plump, robust appearance.
In addition, a diet containing a high amount of refined sugars can cause damage to collagen. The mechanism is through glycation, wherein the sugar molecules in the bloodstream—present from eating a high-sugar food—attach to proteins, forming advanced glycation end products (AGEs). AGEs are toxic to surrounding proteins and can cause collagen to become damaged.
Hypodermis
The hypodermis is the deepest layer of the skin. It is also referred to as the subcutaneous layer, or subcutis. The hypodermis contains blood and lymph vessels, nerves, oil and sweat glands, hair roots, and lots of adipocytes.These adipocytes act as an insulator and shock-absorber to protect tissues underneath, such as muscles and organs.
Touch
Your skin can distinguish between sensations of pain, temperature, vibration, and touch. Nociceptors are nerve cell endings in your skin that can detect painful stimuli. The stimuli can be pressure, temperature, or chemicals. TRPV1 is an ion channel in skin nerve cells that is stimulated by high temperatures and capsaicin—the substance that makes chili peppers spicy.- Meissner corpuscles sense movement across the skin.
- Ruffini endings are responsive to stimuli that make the skin stretch.
- Merkel cells are important in defining the spatial location of touch.
- Pacinian corpuscles sense vibration, specifically high-frequency vibration.
Color
Skin color is determined not only by melanin production and storage but also by carotenoids and blood flow dynamics.Carotenoids can be found throughout the skin, including the epidermis, dermis, and hypodermal adipose tissue. You’re familiar with beta carotene—a carotenoid found in certain vegetables, such as carrots. There are many carotenoids; humans eat as many as 30 different carotenoids, which give our skin a slightly yellowish appearance, particularly in the absence of high concentrations of melanosomes.
UV light from the sun can cause oxidative damage to the skin. Carotenoids in the skin are particularly adept at protecting the skin from this kind of damage.
Skin Color and Disease
Specific skin colors can indicate disease—sometimes very serious disease.Pale skin (pallor) can be indicative of reduced blood flow, as in Raynaud’s syndrome, or a reduced number of red blood cells, as occurs in anemia.
Blue skin, or cyanosis, can be caused by an overabundance of deoxygenated hemoglobin in the blood. Cyanosis can be a symptom of severe heart or lung disease.
Yellow skin can be indicative of jaundice, caused by liver cancer or viral infections of the liver, such as hepatitis. Jaundice can also be caused by Ascaris lumbricoides, a parasite which can block parts of the liver.
Patches of brown skin from hyperpigmentation can indicate Addison’s disease, a condition where the body doesn’t produce enough cortisol.
Finally, areas of abnormal skin color may indicate skin cancer.
There are three main types of skin cancer: squamous cell carcinoma, basal cell carcinoma, and melanoma. Often, these cancers occur in parts of the body that receive a high level of UV exposure; however, these cancers can occur on areas of your skin that receive little sun exposure.
Squamous cell carcinomas may appear as a flat area with a scaly, crusty surface, or as a red nodule. Basal cell carcinomas can appear as a waxy, shiny bump. They can look flat and scar-like or they can present as a bleeding sore that scabs but doesn’t heal. Melanoma may appear as a mole that has changed in color, shape, or size. The mole may also bleed. Melanoma may also appear as a brown spot with speckles of a darker pigment, or portions that appear red, white, or pink.
Getting regular full-body skin exams by a dermatologist is important for ensuring that skin cancer doesn’t grow unnoticed.
Barsh G. S. (2003). What controls variation in human skin color?. PLoS biology, 1(1), E27. https://doi.org/10.1371/journal.pbio.0000027
Bikle DD. Vitamin D: Production, Metabolism and Mechanisms of Action. [Updated 2021 Dec 31]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278935/
Lumen Learning. (n.d.). Layers of the Skin | Anatomy and Physiology. Https://Courses.Lumenlearning.Com/Nemcc-Ap/Chapter/Layers-of-the-Skin/. Retrieved May 15, 2022, from https://courses.lumenlearning.com/nemcc-ap/chapter/layers-of-the-skin/
Pogorzala, L. A., Mishra, S. K., & Hoon, M. A. (2013). The cellular code for mammalian thermosensation. The Journal of neuroscience : the official journal of the Society for Neuroscience, 33(13), 5533–5541. https://doi.org/10.1523/JNEUROSCI.5788-12.2013
Skin cancer - Symptoms and causes. (2020, December 5). Mayo Clinic. Retrieved May 16, 2022, from https://www.mayoclinic.org/diseases-conditions/skin-cancer/symptoms-causes/syc-20377605#:%7E:text=Skin%20cancer%20%E2%80%94%20the%20abnormal%20growth,squamous%20cell%20carcinoma%20and%20melanoma.
Skin cancer - Symptoms and causes. (2020b, December 5). Mayo Clinic. Retrieved May 15, 2022, from https://www.mayoclinic.org/diseases-conditions/skin-cancer/symptoms-causes/syc-20377605