This copy is for your personal, non-commercial use only. Distribution and use of this material are governed by our Subscriber Agreement and by copyright law. For non-personal use or to order multiple copies, please contact The Epoch Times Reprints.
In so many words—and data—the Centers for Disease Control and Prevention (CDC) has quietly admitted that all of the indignities of the COVID-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, and especially the vaccines—all of it failed to control the pandemic.
It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period in 2006. The spread of a new virus with a replication factor R0 of about three, with more than 1 million cases across the country by April 2020 and with no potentially virus-sterilizing vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
COVID-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully two to three weeks later. Thus, management of the COVID-19 pandemic should not have relied upon counts of cases or infections but on the number of deaths, the number of people hospitalized or with serious long-term outcomes of the infection, and serious health, economic, and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities.
Even though the numbers of COVID-19 cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because COVID-19 infection mortality is estimated to range below 0.1 percent in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious “long-COVID” on first infection.
Nevertheless, once the COVID-19 vaccines were rolled out, with a new large wave of the Delta strain spreading across the United States in July–August 2021 even after eight months of the vaccines taken by half of Americans, instead of admitting policy error that the COVID-19 vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates. That didn’t work out too well, as seen when the large Omicron wave hit the country during December 2021–January 2022 despite some 10 percent more of the population getting vaccinated from September 2021 through December 2021.
A typical mandate example: In September 2021, Washington Gov. Jay Inslee issued Emergency Proclamation 21-14.2, requiring COVID-19 vaccination for various groups of state workers. In the proclamation, the stated goal was, “WHEREAS, COVID-19 vaccines are effective in reducing infection and serious disease, and widespread vaccination is the primary means we have as a state to protect everyone ... from COVID-19 infections.” That is, the stated goal was to reduce the number of infections.
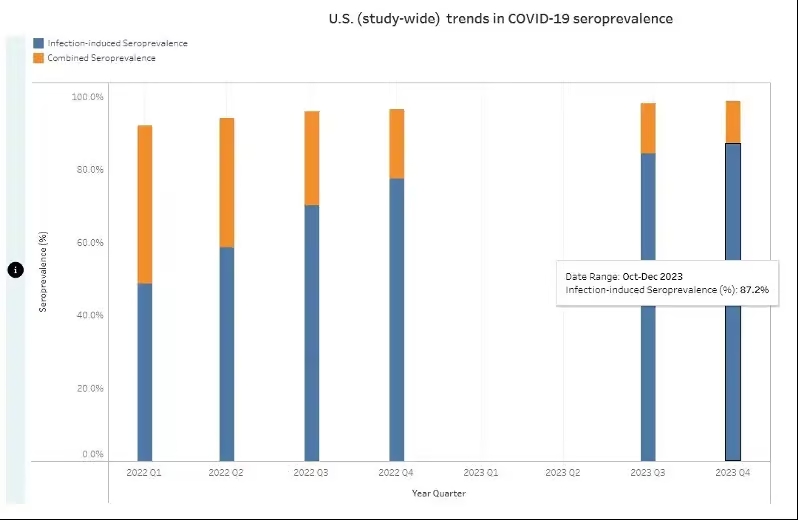
What the CDC recently reported, however, is that by the end of 2023, cumulatively, at least 87 percent of Americans had anti-nucleocapsid antibodies and thus had been infected with SARS-CoV-2. This was in spite of the mammoth, protracted, and booster-repeated vaccination campaign that led to about 90 percent of Americans taking the vaccines.
My argument is that by making policies based on the number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce the spread failed in that 87 percent of Americans eventually became infected anyway.
In reality, neither vaccine immunity nor post-infection immunity was ever fully able to control the spread of the infection. On Aug. 11, 2022, the CDC stated: “Receipt of a primary series alone, in the absence of being up to date with vaccination through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.”
Public health pandemic measures that “wane over time” are very unlikely to be useful for control of infection spread, at least without very frequent and impractical revaccinations every few months.
Nevertheless, infection spread per se is not of consequence, because the count of infections is not and should not have been the main priority of public health pandemic management. Rather, the consequences of the spread and the negative consequences of the policies invoked should have been the priorities. Our public health agencies chose to prioritize a failed policy of reducing the spread rather than reducing the mortality or the lockdown and school and business closure harms, which led to unnecessary and avoidable damage to millions of lives. We deserved better from our public health institutions.
Dr. Harvey Risch is professor of epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine. He received his M.D. from the University of California–San Diego and Ph.D. from the University of Chicago. After serving as a postdoctoral fellow in epidemiology at the University of Washington, Risch was a faculty member in epidemiology and biostatistics at the University of Toronto before coming to Yale.