Florida and Iowa have passed healthcare policy reforms Congress has tried and failed to enact, with new laws that took effect on July 1.
A new Florida law has tightened restrictions on pharmacy benefit managers. These companies, most owned by large insurance companies, are the middlemen in the drug supply chain, exercising significant control over drug pricing and which drugs an insurance company will cover.
Iowa has enacted health insurance reforms, including a measure to prevent insurers from influencing a physician’s decision on where to refer a patient for further treatment.
Despite bipartisan support in Washington for tougher regulation of pharmacy benefit managers, Congress has not passed significant reforms, although some changes were included in the One Big Beautiful Bill Act, according to law firm Mintz.
The Patients Over Profits Act, designed to stop healthcare insurers from buying up and controlling independent medical clinics, was introduced in the U.S. House in 2025 but has not advanced.
The Doctor Knows Best Act, to prohibit health insurance plans from imposing a prior authorization, step therapy protocol, or medical necessity review for any covered healthcare services, was proposed in 2025 but has not been acted upon.


Here is a closer look at these state-level mandates.
Florida Tightens Pharmacy Benefit Managers Rules
Florida’s Drug Prices and Coverage Act, signed by Gov. Ron DeSantis in March, provides new protections for pharmacies when dealing with pharmacy benefit managers.
The law prohibits pharmacy benefit managers from forcing a pharmacy to dispense a drug if the pharmacy benefit manager pays it less than the drug’s cost.
And benefit managers cannot pay their own affiliated pharmacies more than they pay independent pharmacies for the same services.
The law presents a “targeted approach” to regulating pharmacy benefit manager reimbursement practices by placing a blanket prohibition on increasing reimbursements to affiliated pharmacies, according to the Florida Bar.
Also, pharmacies now have a formal way to challenge benefit managers if the payment they receive for a drug is lower than what it actually cost them to buy it.
Pharmacy benefit managers are required to provide a reasonable administrative appeal procedure that allows a pharmacy or pharmacist to challenge the maximum allowable cost pricing information and the reimbursement as being below the acquisition cost.
To reduce paperwork, pharmacies can group multiple claims for the same drug into a single appeal.
Pharmacies have 30 business days to file an appeal after a price update or claim, and pharmacy benefit managers must respond within 30 business days of receiving it.
“This legislation addresses real challenges impacting pharmacies and the patients they serve, and it reinforces what we continue to say at the capitol: Sustainable pharmacy practice is essential to patient access and quality care,” said Eric Larson, president of the Florida Pharmacy Association.
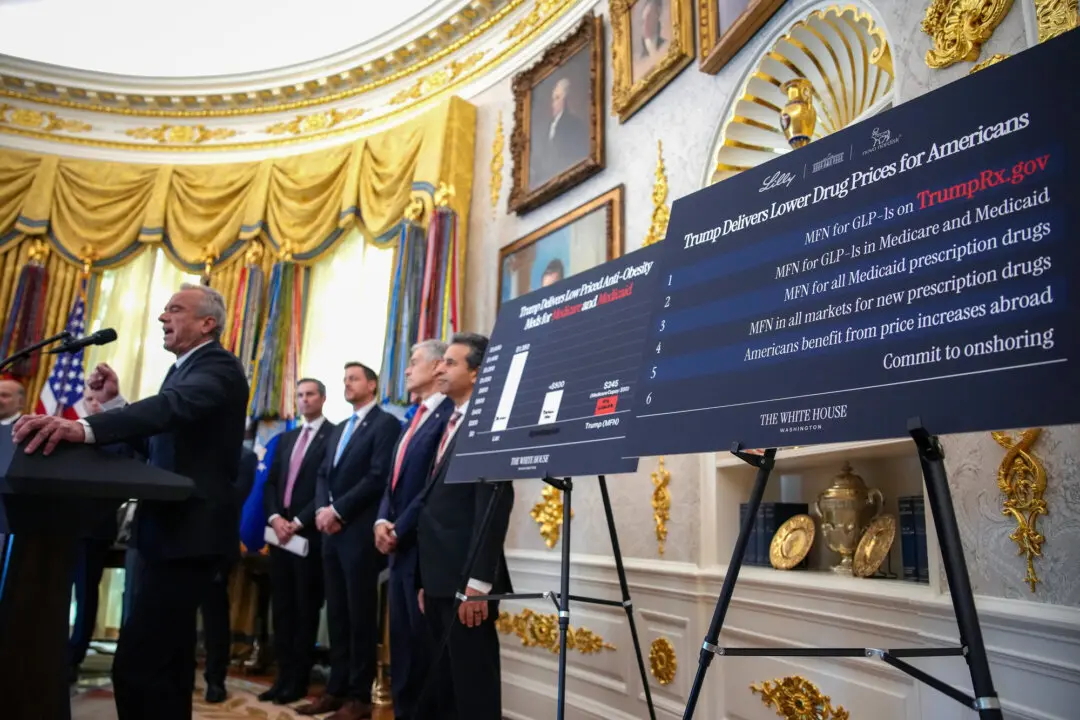
However, Tom Schatz, president of the Council for Citizens Against Government Waste, said prices in the Florida law are based on most-favored-nation pricing, which imports “the worst features of overseas government-run healthcare systems, where treatments are routinely delayed, denied, and restricted.”
“The law would outsource Americans’ healthcare decisions to foreign governments’ one-size-fits-all bureaucratic, socialist judgments,” Schatz said in a February statement.
President Donald Trump signed an executive order in May 2025 to ensure most-favored-nation pricing for the Medicare program.
Iowa Regulates Insurers
A law signed by Iowa Gov. Kim Reynolds on May 13 prevents insurance companies from punishing doctors for referring patients to specialists who might be out of network.
Under the law, an insurance company cannot get involved in or try to influence doctors’ decisions about who they hire or where they send their patients for additional care, a practice known as patient steering.
Insurance companies often steer patients toward their preferred providers, according to the Texas Association of Freestanding Emergency Centers.
Insurers may have a financial interest in directing patients to the cheapest possible care available but have less interest in considering the quality of care or the timeliness of care, said Dr. Eric McLaughlin, an association board member, in a January article.
Chris Mitchell, president and CEO of Iowa Hospital Association, said: “By reducing red tape and improving accountability for insurers, hospitals and providers can spend more time caring for Iowans and less time and expense on paperwork. We are grateful for the strong bipartisan votes this bill received in both chambers.”
The law also bars an insurance company from forcing a healthcare provider to accept a new contract or any changes to an existing one without first giving the provider a chance to discuss and bargain over the terms.
To ensure that patients get fast care for serious conditions, the law removes the prior authorization requirement for recommended cancer screenings and emergency medical conditions that arise while a patient is already hospitalized.
The law also forbids using artificial intelligence as the only basis for rejecting a prior authorization request based on medical necessity.
“This law addresses a high priority for physicians across Iowa—fewer barriers to care and decisions grounded in clinical expertise,” said Dr. Lillian Erdahl, president of the Iowa Medical Society. “By addressing prior authorization challenges and strengthening accountability for insurers, we help ensure patients receive timely, appropriate care.”
Restricting a health carrier’s ability to impose punitive financial incentives on healthcare providers may increase costs to the state of Iowa plan, according to Wellmark Blue Cross and Blue Shield, in an Iowa legislative fiscal note.
In June 2024, Medicare Advantage organizations denied 12 percent of prior authorization requests for skilled nursing services, which help patients recovering from an illness, injury, or surgery, according to a June report from the U.S. Department of Health and Human Services Office of Inspector General.
A notable 95 percent of skilled nursing service denials were overturned on appeal.
Additionally, CVS Health Corp., Humana, and UnitedHealth Group, the three largest Medicare Advantage organizations by enrollment, denied the majority of prior authorization requests for long-term acute care (more than 70 percent) and inpatient rehabilitation (more than 50 percent).
“This raises concerns about whether contractors are receiving appropriate training and oversight from [Medicare Advantage organizations],” the Office of Inspector General said in the report.
In April, the Centers for Medicare and Medicaid Services proposed rules to tighten insurers’ pre-approval timeline and require plans to publicly disclose prior authorization denial rates, appeal outcomes, and detailed reasons for denial.
These rules are set to take effect on Oct. 1, 2027, or Oct. 1, 2028, according to the Centers for Medicare and Medicaid Services proposal.