
Medicare will cover certain GLP-1 drugs for weight reduction at a $50 copay per month starting July 1.
The federal pilot program, known as Medicare GLP-1 Bridge, will expire at the end of 2027.
The program operates outside standard Medicare Part D, which covers prescription drugs, so the Part D deductible does not apply, according to the Centers for Medicare and Medicaid Services.
Beneficiaries pay a flat $50 copay regardless of their coverage in the deductible phase or the initial coverage phase. But low-income subsidies, manufacturer coupons, and other discount programs cannot be used to reduce this copay.
Here is a breakdown of how the program will work
Eligibility
To qualify for the Medicare GLP-1 Bridge, a beneficiary must be enrolled in Medicare Part D, be at least 18 years old, and meet specific clinical criteria at the time they started GLP-1 therapy.
The criteria are based on body mass index (BMI)—a measure of weight relative to height—and other health-condition requirements. People will qualify if their BMI is at or above 35.
Individuals with a BMI of 30 or more can qualify if they have a diagnosis of heart failure, uncontrolled high blood pressure, or chronic kidney disease.
Someone with a BMI as low as 27 can qualify with a diagnosis of pre-diabetes, previous heart attack, previous stroke, or symptomatic peripheral artery disease.
Beneficiaries must have met the clinical criteria when they first started GLP-1 therapy, even if that was before they enrolled in Medicare or before the program’s July 1 launch. So if a patient started the treatment with BMI of 37 and now has a BMI of 34, they would still qualify based on their initial BMI.
Covered Drugs
The pilot program will cover Eli Lilly’s Zepbound (KwikPen) and Foundayo, as well as Novo Nordisk’s Wegovy (injection and tablets) to help beneficiaries manage weight.
More than 16 million Americans have used injectable versions of these GLP-1 medications, with Wegovy capturing more than one-quarter of the market in 2024.
“These treatments are a major medical advancement, but too many seniors are currently unable to access them due to high cost,” Dr. Mehmet Oz, administrator of the Centers for Medicare and Medicaid Services, said in a statement.
The list of covered drugs may be updated while the program is running, according to a statement from the centers.
These drugs will not be covered by the program if beneficiaries have a prescription only to treat a different condition, such as Type 2 diabetes, heart disease, or sleep apnea. In those cases, beneficiaries can continue to get medication through regular Medicare Part D plans.
“Although this is an important first step, patients deserve more than a temporary bridge to care. They deserve sustainable access to comprehensive obesity treatment that recognizes obesity as the chronic disease it is,” said Jacqueline M. Stephens, president of The Obesity Society, in a letter to the federal department.
The Obesity Society encouraged the federal agency to expand access to the full range of FDA-approved obesity medications.
Prior Authorization
A medical provider must submit a prior authorization request and a prescription for the medication to be covered.
The federal agency strongly encourages providers to submit electronically.
A provider does not need to be enrolled in Medicare to submit a prior authorization request, but they must not be on the Preclusion List—providers not receiving payment for Part D drugs.
The federal government uses a single central processor, Humana, to manage the prior authorization, claims adjudication, and payment to pharmacies for the Medicare GLP-1 program.
The prior authorization approval or denial will take up to 72 hours after submission, according to the federal government.
Prior authorization requests will not be accepted or processed before July 1.
Medicare Cost
Chris Klomp, Medicare director at the Centers for Medicare and Medicaid Services, noted that the agency expects initial enrollment to be in the “single-digit millions.”
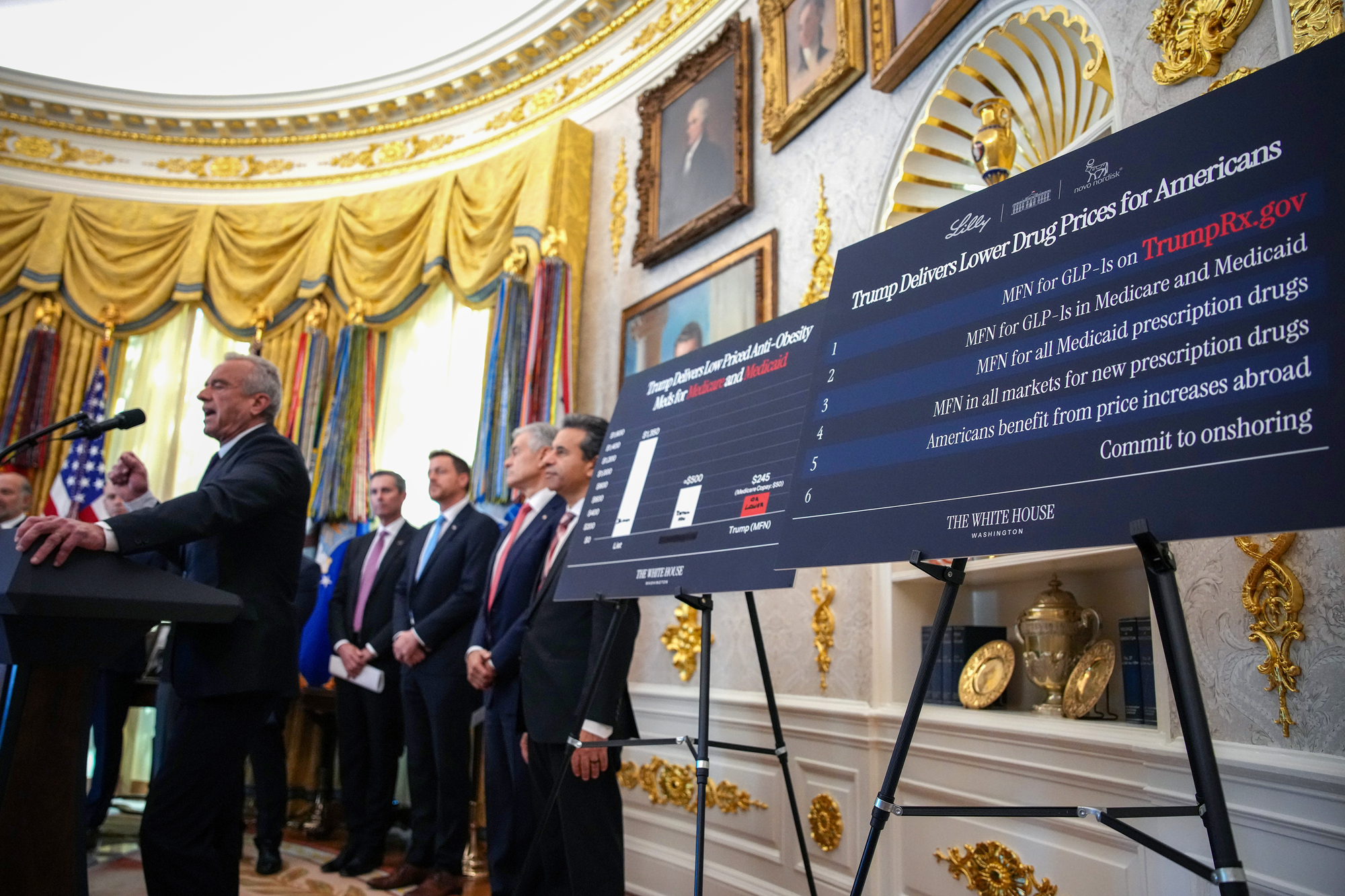
The White House announced pricing deals with multiple pharmaceutical manufacturers in November 2025 to lower domestic prices for drugs, including Zepbound and Wegovy. That set a Medicare price of $245 per month for GLP-1 drugs when prescribed for weight management—far below previous U.S. list prices, which often exceeded $1,000 per month, according to the University of Chicago Medical Center.
Among the nearly 48 million Medicare Part D enrollees in 2023, about 10 million met the clinical criteria in 2023. But fewer than half of them are estimated to be eligible, according to an analysis by health research group KFF.
These 3.8 million Part D enrollees met the clinical criteria and did not have conditions that would qualify for GLP-1 coverage under Part D.
The program cost for Medicare could be $1.3 billion to $3.3 billion if 10 percent to 25 percent of Medicare beneficiaries participate, according to KFF. That estimate assumes that the nearly 4 million estimated eligible beneficiaries start the program in July 2026 and continue through 2027.
If participation instead ranged from 5 million to 7.5 million, the cost to Medicare could be as high as $10 billion, according to KFF.
A May study from the University of Chicago Medical Center projected increased Medicare spending of $18 billion over a decade based on the most-favored-nation price.
“Our model shows that GLP-1 drugs still don’t ‘pay for themselves’ yet at the new price,” David Kim, an author of the study, said in a UChicago Medicine article.
“But we see that the budget impact is much less severe than people have previously anticipated,” he added.
“Ultimately, lower prices for GLP‑1 drugs do strengthen the case for expanding coverage in Medicare, and they also make it more feasible for other payers like Medicaid and private insurers to consider broader coverage,” Kim said.