

My good friend professor Yuri Maltsev died this week and I’ve spent these mourning days recalling our conversations. He was a leading economist in the old Soviet Union, as the top advisor to Mikhail Gorbachev’s chief economist. He defected in 1989 before the Soviet Union fell apart. We became fast friends just after he landed in D.C., and we spent a year or more together collaborating on many projects.
He was a font of amazing stories about how things really worked in the Soviet Union. Contrary to what U.S. economists were claiming until the very end, it was not a rich country with mighty industrial achievements. It was a poor country where nothing worked. There were no replacement parts for most machines including tractors. He doubted that there would ever be a nuclear exchange simply because most Soviet workers knew that the bombs were all for show. If they ever dared press the button, they would most likely blow themselves up.
As the systems of command and control in those states fell apart (Russia, East Germany, Romania, Poland, Czechia, and so on), Yuri was in a position to advise the reforms. To his sadness and contrary to his advice, even though the parties and leaderships collapsed, there was almost no attempt to reform the health-care sectors of these countries. They left them all in place while focusing on things like heavy industry and technology sectors (and here banditry took over).
Yuri saw this as tragic because, to his mind, the corruption of health care in the Soviet Union was central to the disastrous quality of life that the people experienced there. Though doctors were everywhere and minted daily, people who were sick could hardly get effective treatment at all. Most of the best therapeutics were homegrown. People would only go to the doctor much less the hospital if they had no other options. This is because the instant you entered the system, your personhood was left behind and you became part of the modeling target.
All health care was driven by statistical goals, just as with economic production. Hospitals were under strict orders to minimize death or at least not to go over target. That led to a perverse situation. Hospitals would take in the mildly sick but refuse to admit anyone likely to die. If patients in critical care declined too rapidly, the first priority of the hospital was to get them out before they died so as to reduce the amount of death on the premises.
All of this was done in the hope of gaming the vital statistics to make it look like the centralized and socialized health-care systems worked when they clearly did not.
None of this could ultimately hide the vital statistics, which, Yuri explained, truly do tell the story. From 1920 to 1960, life expectancy did increase dramatically though never quite reaching as high as the United States. But after 1960, it began to decline even as it was rising more and more in the United States and in non-communist countries around the world. This continued until the regime finally collapsed, at which point life expectancy began to rise again.
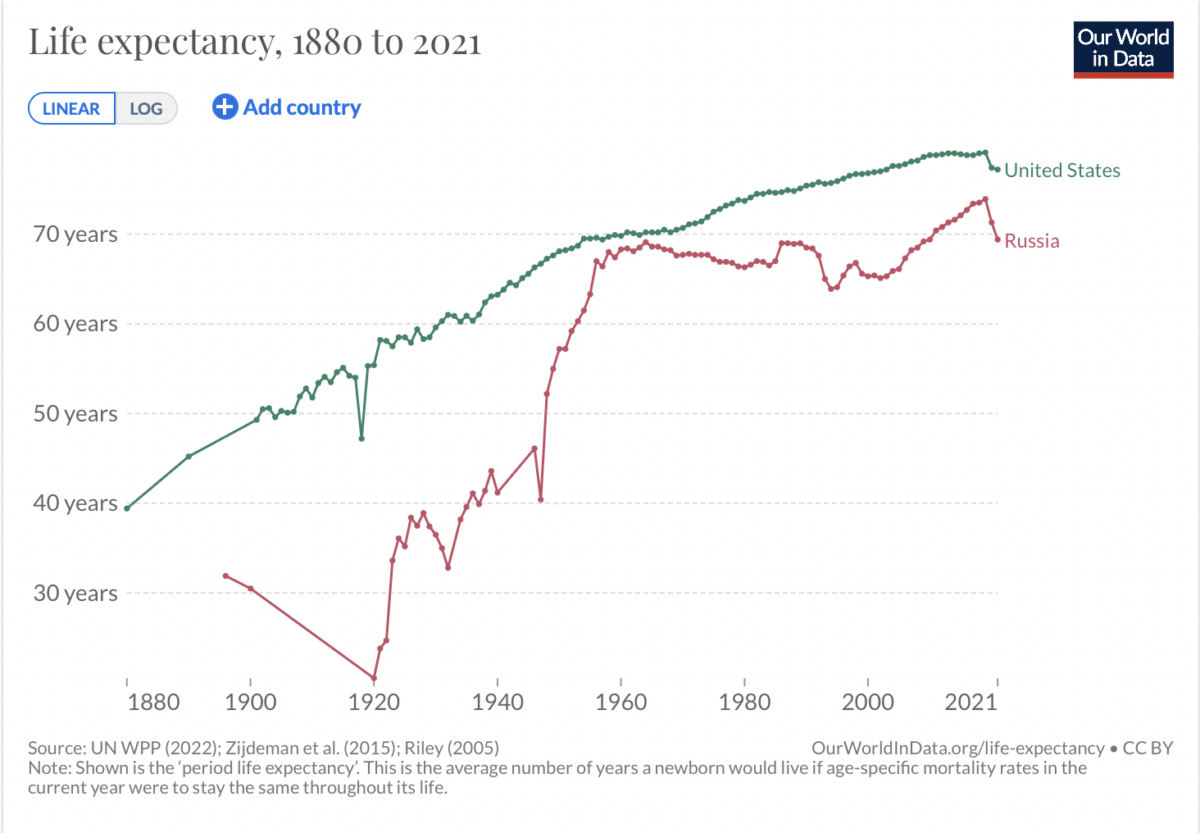
Notice too that life expectancy in both countries has begun to fall again, and dramatically, following pandemic lockdowns and mass vaccination, which is a tragedy that cries out for explanation.
Back to Yuri’s point however: the health-care system and its statistical goals served as a major source of brutality and corruption in Russia. When government gets hold of medical systems, they use them for their own propaganda ends and purposes. That’s true whether the real goals are medical or not.
This happened in both countries following lockdowns, and many others as well. Maybe it is only a short blip or maybe it is the beginning of a long trend of decivilization. Either way, the central plan is not working.
In the United States, in nearly every state, regardless of whether the virus was spreading rapidly with significant medical consequences, hospitals were forcibly reserved only for emergencies and COVID patients. Elective surgeries were out of the question, as were cancer screenings or other routine checkups. This left most hospitals in the country with very few patients and a gutting of their profitability models, leading to furloughs of thousands of nurses during a pandemic.
It also created a situation in which hospitals were desperate for a revenue source. By government legislation, a subsidy was provided to them for COVID patients and COVID deaths, thus incentivizing medical institutions to classify everyone with a positive PCR test as a COVID case, regardless of what else was wrong with the patient.
This began almost immediately. Here is Deborah Birx speaking to the issue on April 7, 2020.
“Under the federal public-health emergency, which begins its fourth year on Friday, hospitals get a 20% bonus for treating Medicare patients diagnosed with Covid-19. … Another incentive to overcount comes from the American Rescue Plan of 2021, which authorizes the Federal Emergency Management Agency to pay Covid-19 death benefits for funeral services, cremation, caskets, travel and a host of other expenses. The benefit is worth as much as $9,000 a person or $35,000 a family if multiple members die. By the end of 2022, FEMA had paid nearly $2.9 billion in Covid-19 death expenses.”
Further, doctors all over the country are facing massive pressure to list as many deaths as possible as COVID deaths.
“These programs create a vicious circle. They establish incentives to overstate the danger of Covid. The overstatement provides a justification to continue the state of emergency, which keeps the perverse incentives going. With effective vaccines and treatments widely available, and an infection fatality rate on par with flu, it’s past time to recognize that Covid is no longer an emergency requiring special policies.”
Maltsev was right about this as with so much else. The further we move away from health care as essentially a doctor/patient relationship, with freedom of choice on all sides, and the more we allow central plans to replace on-the-ground clinical wisdom, the less it looks like quality health care and the less it contributes to public health. The Soviets already tried this path. It did not work. Health-care by modeling and data targeting: we tried it over the last three years with horrible results.
As Maltsev would put it, the need to de-Sovietize medical care applies in every country, then and now.



